The prevalence of diabetic peripheral neuropathy in youth with diabetes mellitus
Article information

Abstract
Purpose
Diabetic neuropathy (DN) is a serious complication in diabetes mellitus. We aimed to determine the prevalence of DN in pediatric-onset diabetes in a tertiary care center and to assess the sensitivity and specificity of monofilament testing and noninvasive screening to diagnose DN compared with the gold standard nerve conduction study (NCS).
Methods
Sixty-five Thai children and adolescents (39 females) diagnosed with diabetes before 15 years of age were included. All subjects were screened for DN by foot and neurological examinations, light touch sensation by 10 g Semmes-Weinstein monofilaments, and the Michigan Neuropathy Screening Instrument (MNSI). NCSs were used as the gold standard for diagnosis of DN.
Results
Fifty-eight patients had type 1 diabetes (T1D), 5 patients had type 2 diabetes, and 2 patients had other types of diabetes. The mean age was 17.7±4.6 years (8–33 years). The prevalence of DN in this cohort was 12.3% by NCS. All subjects were asymptomatic. Mean diabetes duration did not differ between the groups (with DN 8.0±3.0 years vs. no DN 8.2±5.0 years). Notably, one patient with T1D developed DN within 3 years after diagnosis. Poor glycemic control was a significant risk factor for DN. Glycosylated hemoglobin was higher in the DN group (10.6%±2.3% vs. 8.5%±1.6%, P=0.008). The occurrence of diabetic nephropathy was associated with DN (prevalence rate ratio, 4.97; 95% confidence interval, 1.5–16.46). Foot and neurological examinations, monofilaments, and the MNSI failed to detect DN in all subjects with abnormal NCS.
Conclusions
The prevalence of DN in pediatric-onset diabetes is not uncommon but mainly is subclinical. Poor glycemic control is the main risk factor. Noninvasive screening tests for DN exhibited poor diagnostic sensitivity in the pediatric population.
Highlights
· The prevalence of diabetic neuropathy in pediatric-onset diabetes in our Thai cohort was 12.3%, but is mainly subclinical. Noninvasive screening test for early diabetic neuropathy had poor diagnostic sensitivity in the pediatric population.
Introduction
Diabetic neuropathy (DN) is a serious chronic complication of diabetes mellitus, with distal symmetrical polyneuropathy being the most common manifestation [1]. A prevalence rate of diabetic peripheral neuropathy in children in previous studies varied from 7% up to as high as 32% [1-7] depending on the screening tools, the population of the study, and the definition of DN. Data of DN in pediatric-onset diabetes in Asian populations is limited. Recommendations regarding the timing and interval to screen DN differ between professional guidelines [8,9]. However, DN screening is not common in routine practice of pediatric diabetes clinics.
Poor glycemic control is the most important risk factor of DN. Other factors remain controversial. Hajas et al. [3] reported the main contribution factors for the increasing prevalence of DN as poor glycemic control, duration of diabetes, and older age. Moreover, Jaiswal et al. [2] determined that smoking, high diastolic blood pressure, obesity, increased low-density lipoprotein cholesterol (LDL-C) and triglycerides, and lower high-density lipoprotein cholesterol (HDL-C) were risk factors of DN in youths.
There are several methods used for screening DN. The Michigan Neuropathy Screening Instrument (MNSI) and 10-g monofilaments are widely used to screen DN in adults, but these tools have been less studied in children and adolescents. The accuracy of DN screening tools in children and adolescents is variable [10]. While the nerve conduction study (NCS) remains the gold standard for diagnosis of DN, it is rarely performed in children and youth.
The aims of our study were to explore the prevalence of DN in children and adolescents with pediatric-onset diabetes and its risk factors and to explore the sensitivity and specificity of monofilament testing for light touch sensation and MNSI compared with the NCS for diagnosis of DN.
Materials and methods
A total of 65 Thai children and adolescents (39 females and 26 males) diagnosed with diabetes before 15 years of age and treated in the pediatric diabetic clinics at King Chulalongkorn Memorial Hospital, Bangkok, Thailand, from January to December 2018 were enrolled in this study. The study group consisted of 58 patients with type 1 diabetes (T1D), 5 patients with type 2 diabetes (T2D), and 2 patients with other type of diabetes (neonatal diabetes, pancreatic hemochromatosis). In the T1D group, we enrolled patients who had a duration of diabetes of at least 3 years and had received basal bolus insulin regimen. In the T2D group, patients were enrolled at any time during the duration of diabetes. We excluded patients with steroid-induced diabetes and patients who had a history of neurological disease or use of any medication with known effects on peripheral nerve function.
Data were obtained from patient medical records and included age, sex, duration of diabetes, weight, height, treatment regimen, current glycosylated hemoglobin (HbA1c) level at the most recent visit, and current lipid profiles (cholesterol, triglycerides, LDL-C, and HDL-C) as assessed within one year of the study. Serum level of C-reactive protein (CRP) was determined using nephelometry methods (Siemens, BN prospect). All subjects were scheduled for routine annual screenings for diabetic retinopathy by ophthalmologists. Morning spot urine samples were collected for screening for diabetic nephropathy. The presence of microalbuminuria was defined as urine microalbumin/creatinine ≥30 mg/g in males and ≥42 mg/g in females [9].
Symptoms of DN were screened by the Michigan Neuropathy Screening Instrument Questionnaire (MNSIQ) [11]. The MNSIQ consisted of 15-item self-administered questionnaires that were translated and validated into Thai [12], A score ≥ 4 was considered abnormal [13].
The foot and neurological examinations for DN were divided into 2 main parts. In the first part, light touch sensation by 10-g Semmes-Weinstein monofilaments was performed by a pediatric endocrinologist. The monofilament test was performed according to the American Diabetes Association recommendation in 2008 to screen at 4 sites per foot - the hallux and the first, third, and fifth metatarsal heads [14]. The subjects are tested for perception of pressure at the correct site [14]. For the second part, MNSI examination (MNSIE) was assessed by foot inspection (excessively dry skin; callous formation; fissures; and frank ulceration or deformities including flat feet, hammer toes, overlapping toes, hallux valgus, joint subluxation, prominent metatarsal heads, medial convexity [Charcot foot], and amputation), vibration sensation (using a 128-Hz tuning fork), muscle stretch reflex (ankle reflex), and monofilament testing. A score ≥ 2.5 was defined as abnormal [13].
The electrophysiological study was performed following the American Association of Electrodiagnostic Medicine guidelines with a Medelec Synergy EMG/EP System (software version 11, Oxford Instruments plc, Abingdon, UK). Nerve conduction studies were performed in all subjects on the sural and common peroneal nerves in both lower extremities by an experienced physician who was blinded to the subject's information. Conduction velocities were determined bilaterally on the sural and common peroneal nerves. The presence of "DN" was defined as abnormal nerve conduction velocity (NCV) in one of 4 examined nerves (right sural nerve, left sural nerve, right common peroneal nerve, and left common peroneal nerve). Electrophysiological values were considered abnormal if they exceeded the mean±2 standard deviation of the healthy control group. NCVs less than 35 m/sec for the sural nerve and less than 40 m/sec for the common peroneal nerve were considered abnormal based on our standard for the Thai population [15]. We defined "confirmed DN" as the presence of abnormal NCS with symptoms or signs of neuropathy. “Subclinical DN” was defined as the presence of abnormal NCS without signs or symptoms of neuropathy [16].
1. Statistical method
Data analysis was performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Descriptive statistics were described as number and percentage, mean and standard deviation, or median and range. Multiple logistic regression analysis was used to assess the risk factors for DN. Fisher exact test was used to determine an association between other complications and DN presented by prevalence rate ratio (PRR). The diagnostic performance of the screening tests (10-g monofilament, MNSI, and CRP) was presented as sensitivity, specificity, positive predictive value, and negative predictive value. A P-value less than 0.05 was considered statistically significant.
2. Ethical statement
This study was performed according to the Helsinki Declaration and approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (COA No. 144/2018). Written informed consent was obtained from all subjects.
Results
A total of 65 patients (39 females) was included in this cross-sectional study. Demographic data were shown in Table 1. Mean age was 17.8±4.6 years (range, 8–33 years). Mean HbA1c was 8.8%±1.8%, while the median duration of diabetes was 7 years (range, 1–22 years). Of the 65 subjects, 8 (12.3%) had abnormal NCS results (6 with T1D, 1 with T2D, and one each with hemochromatosis-induced diabetes). All subjects with abnormal NCV were clinically asymptomatic. Therefore, we defined them as having subclinical DN. Table 2 demonstrates the characteristics of patients with DN. In the T1D group, duration of diabetes was 7.5±0.3 years. Notably, one patient had developed DN in only 3 years since diagnosis. All patients with DN exhibited poor glycemic control, particularly those in the T1D group (mean HbA1c was 11.2%±2.3%).
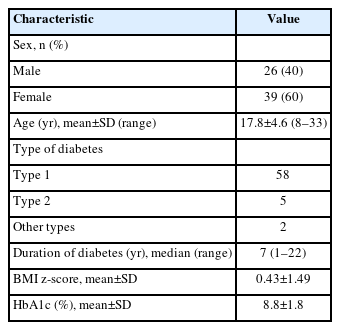
Characteristics of all subjects in this study (n=65)
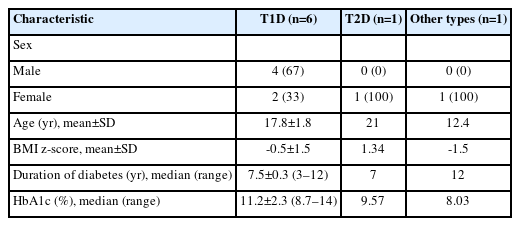
Characteristics of 8 patients with diabetic neuropathy diagnosed by nerve conduction study
Regarding the NCS results, we found that 5 patients had motor neuropathy, 2 had both sensory and motor neuropathy, and 1 had only sensory neuropathy. NCVs were significantly decreased in all tested nerves (both sural and common peroneal nerves) in patients diagnosed with DN compared to the normal group, as shown in Table 3.
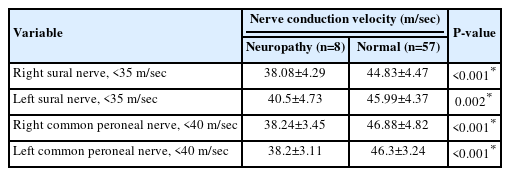
Results of nerve conduction study
Multiple logistic regression analysis was used to verify the independent risk factors of neuropathy (Table 4). The results showed poor glycemic control (HbA1c level) as the strongest risk factor of DN. Adjusted odds ratio (OR) for HbA1c was 1.65 (95% CI, 1.04–2.61; P=0.032). HbA1c level was significantly higher in the group with DN (10.6%±2.3% vs. 8.6%±1.6%, P=0.008). LDL-C tended to be higher in the neuropathy group but did not reach statistical significance (146±54 mg/dL vs. 122±34 mg/dL, P=0.099). The body mass index z-score was lower in the neuropathy group, but after adjusting for the OR, it did not reach statistical significance (-0.47±1.53 vs. 0.56±1.22, P=0.041). There were no significant differences in age, sex, type of diabetes, and duration of diabetes between the groups with or without neuropathy.
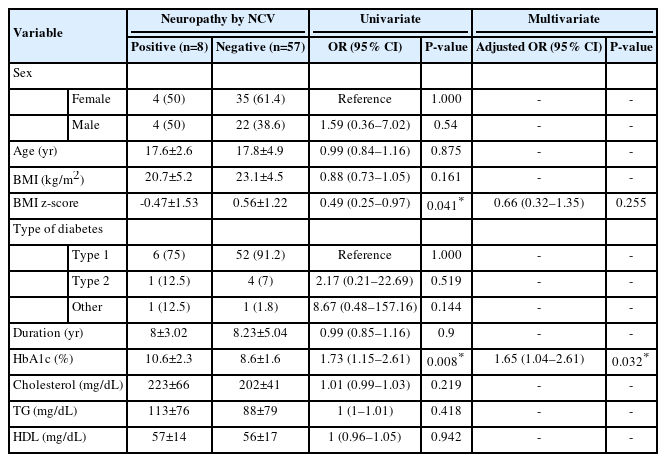
Factors associated with diabetic neuropathy by logistic regression analysis
By Fisher exact test, a statistically significant relationship was observed between diabetic nephropathy and diabetic retinopathy as demonstrated by the PRR (95% CI) of 4.97 (1.5–16.5), P=0.035 (Table 5). The presence of dyslipidemia and diabetic retinopathy had no significant association with DN.

An association of diabetic neuropathy with other diabetes-related complications
The diagnostic performance of a 10-g monofilament test, MNSIQ, and MNSIE could not be calculated because all noninvasive screening tests were negative in all subjects with abnormal nerve conduction studies. Serum CRP level was elevated in 1 of 7 patients with DN. Therefore, our results suggest that 10-g monofilament testing, MNSI, and CRP exhibited low diagnostic performance for detection of peripheral neuropathy in children and adolescents with diabetes.
Discussion
In this cross-sectional study, the prevalence of DN in pediatric-onset diabetes was 12.3%. All patients were clinically asymptomatic, and poor glycemic control was the main risk factor. The presence of diabetic retinopathy was associated with DN. We determined that a 10-g monofilament test, MNSI, and CRP had low diagnostic performance for detection of peripheral neuropathy in children and adolescents with diabetes.
The prevalence of DN in our study was lower than in previous studies that used the NCS to diagnose DN. Hajas et al. [3] reported a DN prevalence of 24.2% in 62 young patients with T1D, aged 3–28 years with a mean HbA1c of 8.7%. Similarly, most cases (11 of 15) of DN were subclinical. Interestingly, there was an increase in DN prevalence from 24.2% to 62.9% during the 10-year follow-up. The authors determined that long-term poor glycemic control was a strong factor in rapid subclinical DN progression.
Lee et al. [4] performed a 5-year follow-up NCS in 37 patients, aged 3–19 years with new-onset T1D and found that 12 of the 37 patients (32.4%) had evidence of polyneuropathy without clinical signs/symptoms at initial diagnosis. The percentage of abnormal NCV increased over a 5-year follow-up. The authors found that duration of diabetes and poor glycemic control were the most important risk factors of DN.
There is controversy regarding the prevalence of DN in pediatric populations due to the lack of clear consensus recommendations for diagnosis, and there are a very limited number of large studies in the pediatric age group. In addition, there have been no clear cutoff values from NCS to define abnormal conduction velocities in the pediatric population. In this study, we used the standard obtained by measuring the healthy Thai adult population since previous studies suggested that nerve conduction values were not different between adults and children older than 5 years due to a maturation of axon diameter and thickening of myelin [17,18].
Up to now, there have been no consensus guidelines for early detection of subclinical DN in young patients with diabetes. All patients in the present study who had subclinical neuropathy were older than 15 years. The shortest duration in patients with neuropathy was 3 years from initial diagnosis. Therefore, these data findings support the current professional guidelines to begin screening for DN in T1D at age >10 years [8,9]. and also support the reduction of diabetes duration from 5 years to 2–5 years to initiate screening. In line with previous studies, HbA1c is the strongest risk factor of DN. Another possible risk factor is LDL-C, even though it did not reach statistical significance due to a small sample size.
In the DN group, most individuals had only motor neuropathy. Two longitudinal studies found that DN occurred at the onset of diabetes and after 5 and 10 years [3,4]. Solders et al. [19] demonstrated that DN can be detected at diagnosis in ~25% of cases with involved sural nerves. After 2, 5, and 10 years of follow-up, the conduction velocity of sural nerves appeared to be improved after glycemic control. On the other hand, peroneal nerves were normal in most patients at diagnosis, but after 10 years of follow-up, the conduction velocity of peroneal nerves worsened over time. Similarly, Lee et al. [4] performed a 5-year follow-up of DN in children with newly diagnosed T1D and demonstrated similar results.
From our study, all noninvasive screening tests for DN exhibited poor diagnostic sensitivity in the pediatric population. These data findings were consistent with previous studies. Jaiswal et al. [2] screened for DN by MNSI in 1,734 youths with T1D and only detected neuropathy in 7% of the study population.
Currently, there are no specific treatments for DN in children and adolescents. The Diabetes Control and Complications Trial/observational Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) and other trials have demonstrated that intensive control designed to achieve near-normal glycemia is essential for preventing or delaying the progression of DN in T1D, but that glycemic control is modestly effective for T2D [20,21]. In the DCCT/EDIC study, multiple injections were performed 3 or more times a day to achieve the targeted HbA1c [21,22]. Multiple nutritional factors have been involved in the pathogenesis of DN including vitamin B12, vitamin A, and pyridoxine deficiencies. However, the benefit of supplementation remains controversial. Adequate and healthy nutrition is recommended [23]. Aldose reductase has been used in research studies with unproven benefits [23]. Pregabilin and duloxetine have been approved to treat painful DN in adults [24] but not in children. Obesity and dyslipidemia are emerging risk factors for DN in adults and in pediatric studies [1]. Youths with diabetes should be advised on nutrition, weight control, and exercise as well as avoiding smoking and alcohol use to eliminate some modifiable risk factors.
In conclusion, DN in pediatric-onset diabetes is not uncommon but is mainly subclinical. Poor glycemic control is the main risk factor. Noninvasive screening tests for DN exhibited poor diagnostic sensitivity in the pediatric population.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was supported by the Ratchadapisek-sompotch Fund (RA61/030 to T.S.), Faculty of Medicine, Chulalongkorn University.
Data availability
The data that support the findings of this study can be provided by the corresponding author upon reasonable request.
Author contribution
Conceptualization: PS, TS; Data curation: PS, JB, TS; Formal analysis: PS, JB, TS; Funding acquisition: TS; Methodology: PS, JB, TS; Project administration: PS, TS; Visualization: PS, TS; Writing - original draft: PS, TS; Writing - review & editing: JB, TS
Acknowledgements
We would like to thank the patients for their participation in this study.