The association between C-reactive protein, metabolic syndrome, and prediabetes in Korean children and adolescents
Article information

Abstract
Purpose
Metabolic syndrome (MetS) is a state of chronic inflammation, and high-sensitivity C-reactive protein (hsCRP) indicates inflammation. This paper evaluates the associations between hsCRP and MetS and its components in Korean children and adolescents.
Methods
We analyzed the data of 1,247 subjects (633 males, 14.2±2.7 years) from the Korea National Health and Nutrition Examination Survey 2016–2017. This study defined MetS and its components using the modified National Cholesterol Education Program-Adult Treatment Panel III (NCEP-ATP III) criteria.
Results
The mean hsCRP level was 0.86±1.57 mg/dL (median and interquartile range: 0.37 and 0.43 mg/dL). Subjects with MetS had higher hsCRP level than subjects without MetS (geometric mean: 1.08 mg/dL vs. 0.46 mg/dL, p<0.001). With a higher quartile value of hsCRP, the prevalence of MetS increased. Compared to the lowest quartile, the odds ratio (OR) for MetS in the highest quartile was 7.34 (3.07–17.55) after adjusting for age and sex. In the top quartile of hsCRP, the risk of abdominal obesity and low HDL was high after adjusting for age, sex, and other components of MetS. Additionally, the OR for prediabetes (HbA1c ≥5.7%) in the highest quartile was 2.70.
Conclusions
Serum hsCRP level was positively associated with MetS and prediabetes using NCEP-ATP III criteria. Among the MetS components, abdominal obesity and low HDL were highly correlated with hsCRP in Korean children and adolescents.
Highlights
· Serum hsCRP level was positively associated with MetS and prediabetes using NCEP-ATP III criteria. The odds ratio for MetS in the highest quartile was 7.34, and for prediabetes (HbA1c ≥5.7%) was 2.70.
Introduction
Cardiovascular disease (CVD) is a leading cause of death worldwide, including in Korea [1,2]. Metabolic syndrome (MetS), a clustering of cardiovascular risk factors, is associated with the global epidemics of CVD and type 2 diabetes mellitus (T2DM). In adults, the risk for CVD is increased approximately three-fold in subjects with MetS. The hazard ratio for subjects with MetS has been reported as 1.37 for mortality from CVD after adjustment for other confounders [3,4]. Furthermore, MetS in childhood predicts adult MetS and T2DM 25 to 30 years later [5]. However, it is not easy to diagnose MetS in children because many different criteria have been used in its multiple definitions. Further complicating diagnosis are the various references and cutoff values of its 5 components.
MetS is a state of chronic low-grade inflammation; measurements of the circulating levels of the inflammatory molecules might provide diagnostic and therapeutic approaches to modulate or alter disease progression [6].
High-sensitivity C-reactive protein (hsCRP), an inflammation biomarker, has emerged as an independent predictor of CVD and T2DM development [7,8]. Subjects in the top quartile for hsCRP level have shown an odds ratio (OR) of 1.5 for major cardiovascular events compared to those in the lowest quartile after adjusting for established risk factors [5]. Furthermore, the hazard ratios for T2DM in the highest CRP tertile compared to the lowest have been recorded as 2.80 in Korean women and 1.67 in men [8].
In a population-based study, Ford et al. [9] used data from the NHANES 1999–2000 to first report that C-reactive protein (CRP) was higher in children and adolescents who had MetS than in those who did not. Recently, Shin et al. [10] reported the association between MetS and hsCRP using International Diabetes Federation criteria in Korean children and adolescents. Thus, we aimed to examine the associations between serum hsCRP level and the prevalence of MetS and its components using the modified National Cholesterol Education Program— Adult Treatment Panel III (NCEP-ATP III) in Korean children and adolescents.
Materials and methods
1. Subjects
We performed a cross-sectional analysis using data from the Korea National Health and Nutrition Examination Survey (KNHANES) 2016–2017. Detailed information about the methods and procedures of this survey is available to the public on the KNHANES website (http://knhanes.cdc.go.kr) [11]. In short, the survey consists of a health questionnaire, a health examination, and a nutritional assessment using a stratified, multistage probability sampling design of the noninstitutionalized Korean population. Written informed consent was obtained from all participants or parents of participants before the study began. The KNHANES was conducted following ethical approval by the Institutional Review Board of the Korea Centers for Disease Control and Prevention.
In KNHANES 2016–2017, the data of 1,649 children and adolescents aged 10–19 years were available. Therefore, we limited our analyses to the subjects with serum hsCRP data and complete information concerning MetS components (n=1,400). Among them, 40 subjects who had fasted fewer than 8 hours were excluded, as were 11 subjects with chronic diseases like congenital heart disease and rheumatoid arthritis. In addition, subjects with known diabetes and individuals taking antihyperlipidemic or anti-diabetic medications were excluded. Finally, current smokers (n=73) were excluded. Thus, 1,247 subjects (633 males, 614 females) were included in the final analysis.
2. Measurements
Height and body weight were assessed by trained experts to the nearest 0.1 cm using Seca 225 (Seca, Hamburg, Germany) and to the nearest 0.1 kg using GL-6000-20 (G-tech, Seoul, Korea). Waist circumference (WC) was measured at the midline between the lower rib margin and the iliac crest to the nearest 0.1 cm. Systolic blood pressure (SBP, mmHg) and diastolic blood pressure (DBP, mmHg) were recorded 3 times from the right upper arm using a calibrated sphygmomanometer (Baumanometer Desk Model 0320, Baum, New York, NY, USA) and an appropriately sized cuff. The mean of the last 2 values was used for analysis.
After the participants had fasted for at least 8 hours, blood samples were collected, immediately processed, refrigerated, and transported to a central laboratory (NeoDin Medical Institute, Seoul, Korea) for analysis within 24 hours. hsCRP was measured with immunoturbidimetry using Cobas (Roche, Mannheim, Germany). Total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), and glucose were measured enzymatically using a Hitachi 7600 automatic analyzer (Hitachi, Tokyo, Japan). HbA1c was measured using a Tosoh Automated Glycohemoglobin Analyzer (HLC-723G8, Tosoh Bioscience, Japan). Low-density lipoprotein cholesterol (LDL-C) was determined using Friedewald’s equation.
3. Definitions of MetS and prediabetes
This study defined MetS and its components according to the modified NCEP-ATP III [12]. In addition, subjects with MetS had to meet 3 of the following 5 criteria: abdominal obesity (WC ≥ age/sex-specific 90th percentile according to the 2007 Korean growth charts) [13]; hypertriglyceridemia (TG ≥ 110 mg/dL); low HDL-C (HDL-C ≤ 40 mg/dL); high blood pressure (SBP or DBP ≥ age/sex/height-specific 90th percentile) [14]; and hyperglycemia (fasting glucose ≥ 100 mg/dL). Further, subjects with HbA1c ≥ 5.7% were considered prediabetic, and those with LDL-C ≥ 130 mg/dL were deemed to have abnormal LDL-C [15,16].
4. Statistical analyses
Normally distributed variables are presented as the means± standard deviations, while categorical variables are presented as percentages (%). Differences between the 2 groups were assessed using a t-test. In addition, differences among hsCRP quartiles were tested using analysis of variance for continuous variables and the chi-square test for proportions. Because the distributions of hsCRP and TG were highly skewed, this variable was natural log-transformed for the analyses.
The prevalence of MetS and its components were calculated for each quartile of hsCRP level. The lowest, second, third, and highest hsCRP quartiles were defined as Q1 (<0.27 mg/dL), Q2 (0.27–0.37 mg/dL), Q3 (0.37–0.70 mg/dL), and Q4 (≥0.70 mg/dL), respectively. In the United States (US) youth, the percentage of children and adolescents with an elevated concentration of CPR (>0.3 mg/dL) was almost 4 times higher among those with MetS than those without MetS [9]; we quoted this value as the cutoff.
To examine the association between MetS and the hsCRP level, we conducted logistic regression analyses adjusting for age and sex (Model-1). Also, we further conducted several logistic regressions to examine the associations between each component of MetS and hsCRP level after adjusting for age, sex, and other components of MetS as dichotomized variables (Model-2). The ORs and 95% confidence intervals for MetS and MetS components (as well as prediabetes and abnormal LDL-C) were determined according to hsCRP quartile, with the lowest quartile (Q1) serving as the reference. All analyses were conducted using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). A P-value of <0.05 was considered statistically significant.
Results
1. Clinical characteristics of study subjects
The anthropometric and laboratory characteristics of the study subjects with or without MetS are summarized in Table 1. Among the 1,247 subjects (mean age, 14.2±2.7 years), the prevalence of MetS was 6.1% (7.4% in male subjects and 4.7% in female subjects; P=0.046). The contributing factors of MetS of abdominal obesity, hyperglycemia, high blood pressure, hypertriglyceridemia, and low HDL-C were observed in 11.9%, 12.1%, 14.5%, 21.2%, and 11.3% of the subjects, respectively.

Anthropometric and laboratory characteristics of the study subjects by metabolic syndrome
In total, across the subjects, the hsCRP level ranged from 0.15 to 16.9 mg/dL (mean, 0.86 mg/dL; geometric mean, 0.48 mg/dL). Males had higher hsCRP level than females (geometric mean: 0.52±1.04 vs. 0.44±1.04, P=0.001). Subjects with MetS had higher hsCRP level than subjects without MetS (mean: 1.88 mg/dL vs. 0.80 mg/dL, P<0.001; geometric mean: 1.12 mg/dL vs. 0.45 mg/dL, P<0.001). Subjects with MetS had higher body mass index (BMI), HbA1c, TC, and LDL-C compared to those without MetS.
2. Correlations between serum hsCRP level and cardiometabolic parameters
Serum log hsCRP level correlated significantly (all, P<0.01) with BMI (r=0.44), WC (r=0.43), SBP (r=0.16), DBP (r=0.11), HDL-C (r=-0.23), FPG (r=0.10), log TG (r=0.10), HbA1c (r=0.16), and LDL-C (r=0.07). No significant correlation was observed between serum log hsCRP level and age (r=0.05, P=0.06) or TC (r=0.01, P=0.62).
3. Adjusted ORs of MetS and its components according to hsCRP quartile
The mean hsCRP level was 0.86±1.57 mg/dL (median and interquartile range: 0.37 and 0.43 mg/dL). To further evaluate each MetS component, subjects were divided into quartiles according to serum hsCRP level. The prevalence of MetS according to hsCRP quartile is depicted in Fig. 1.
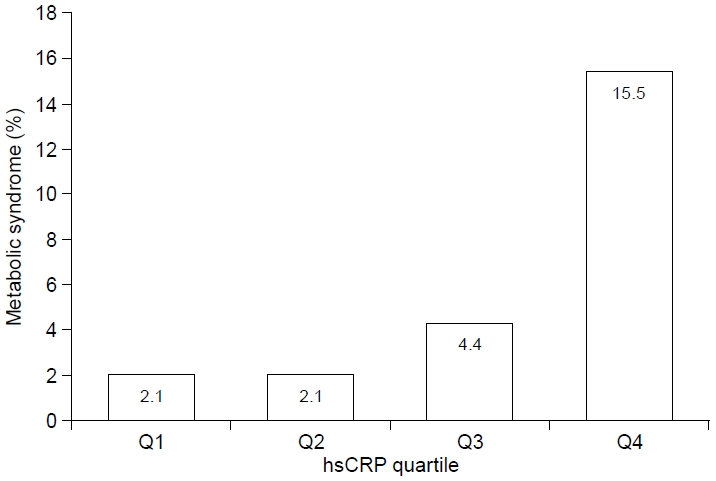
The prevalence of MetS according to hsCRP quartile. The prevalence of MetS in Q1, Q2, Q3, and Q4 was 2.1%, 2.1%, 4.4%, and 15.5%, respectively. MetS, metabolic syndrome; hsCRP, high-sensitivity C-reactive protein.
The prevalence of MetS in Q1, Q2, Q3, and Q4 was 2.1%, 2.1%, 4.4%, and 15.5%, respectively. The prevalence of MetS in subjects who had hsCRP>0.3 mg/dL was 20.0% (14 of 70), and that in those who had hsCRP≤0.3 mg/dL was 5.3% (62 of 1,177). According to quartile, the prevalence of MetS components, prediabetes, and abnormal LDL-C is summarized in Table 2. The prevalence of abdominal obesity and low HDL-C was significantly higher in Q3 and Q4 compared to Q1. In addition, the prevalence of hypertriglyceridemia and prediabetes was significantly higher in Q4 compared to Q1. The numbers of MetS components by quartile were 0.46±0.74, 0.51±0.79, 0.71±0.88, and 1.16±1.22, respectively (P<0.001).

The prevalence of metabolic syndrome components, prediabetes, and abnormal LDL-C according to hsCRP quartiles
The adjusted ORs of MetS and MetS components according to hsCRP quartile, after controlling for the previously mentioned confounders, are presented in Table 3. Compared to Q1, the OR for MetS in Q4 was 7.34 (3.07–17.55) after adjusting for age and sex (Model-1). The ORs for abdominal obesity and low HDL-C in Q4 were 8.43 (4.17–17.05) and 2.46 (1.31–4.61), respectively, after adjusting for age, sex, and other components of MetS (Model-2). The OR of MetS in subjects who had hsCRP >0.3mg/dL compared to those who had hsCRP ≤0.3 mg/dL was 4.09 (1.90–8.80).

Adjusted odds ratios (95% confidence interval) of metabolic syndrome (and its components) according to the hsCRP quartiles
4. Adjusted ORs of prediabetes according to hsCRP quartile
The prevalence of prediabetes (HbA1c≥5.7%) according to hsCRP quartile is depicted in Fig. 2. For Q1, Q2, Q3, and Q4, the prevalence of prediabetes was 6.3%, 8.3%, 8.0%, and 15.0%, respectively. The prevalence of prediabetes in subjects who had hsCRP>0.3 mg/dL was 21.4% (15 of 70), and it was 8.7% (102 of 1,167) for those who had hsCRP ≤0.3 mg/dL. Compared to Q1, the OR for prediabetes in Q4 after adjusting for age and sex was 2.70 (1.51–4.83) (Model-1). The OR decreased to 2.06 (1.10–3.87) but remained significant after adjusting for age, sex, abdominal obesity, high blood pressure, hypertriglyceridemia, and low HDL-C (Model-2). The OR of prediabetes in subjects who had hsCRP >0.3 mg/dL compared to those who had hsCRP ≤0.3 mg/dL was 2.85 (1.55–5.22).
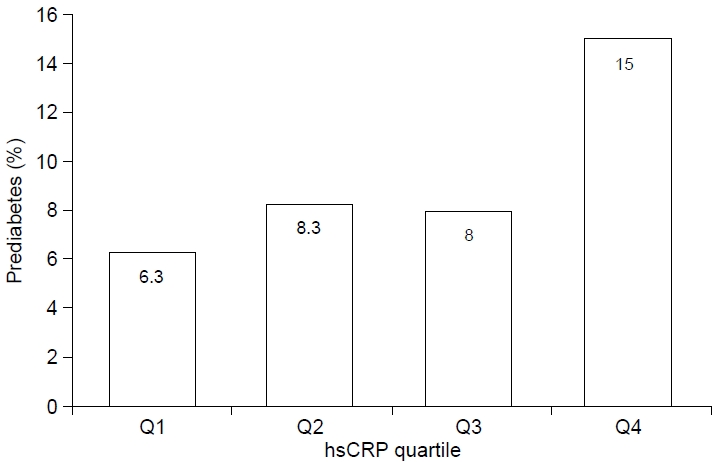
The prevalence of prediabetes (HbA1c≥5.7%) according to hsCRP quartile. For Q1, Q2, Q3, and Q4, the prevalence of prediabetes was 6.3%, 8.3%, 8.0%, and 15.0%, respectively. hsCRP, high-sensitivity C-reactive protein.
Discussion
This nationally representative sample of Korean children and adolescents found that MetS was prevalent among subjects with high hsCRP level using NCEP-ATP III criteria. Even after adjusting for confounding factors in logistic regression, the OR of MetS in subjects within the highest quartile of hsCRP level was 8.41. We also found that not only was abdominal obesity significantly associated with hsCRP, but also was low HDL-C. Also, prediabetes was shown to be associated with hsCRP after adjusting for confounding factors. Thus, our results confirmed the association of hsCRP and MetS in Korean children and adolescents using NCEP-ATP III as well as IDF criteria. This result provides evidence that hsCRP is related to MetS regardless of the definition of MetS.
In the face of the global epidemics of CVD and T2DM, tools are needed to identify the future severity and aggression of these diseases. One tool is MetS, a cluster of CVD risk factors, including central obesity, hypertension, increased fasting blood glucose, high level of TG, and low HDL-C. Another developed tool is obesity-related inflammation as measured by interleukin-6, tumor necrosis factor, and hsCRP levels [17-19]. In adults, higher hsCRP level has been linked to risk of MetS, CVD, and T2DM [20]. Subjects within the highest quartile or quintile have shown adjusted relative risk of 2.3–4.8 for CVD factors such as obesity, age, and smoking [21]. In Korean adults, subjects with high hsCRP (defined as > 75th percentile, 1.43 mg/dL for men and 1.20 mg/dL for women) have been shown to have adjusted relative risk of 2.50 for developing MetS after a 6-year follow-up. Thus, hsCRP can be used for global CVD and T2DM risk prediction in adults with MetS [22].
This study confirmed previous findings of close association between increased level of hsCRP and MetS and its components (abdominal obesity and low HDL-C) in Korean children and adolescents. Ford et al. [9] first reported that CRP was higher among US youth who had MetS than in those who did not (geometric mean: 1.8 mg/dL vs. 0.4 mg/dL). They showed that only abdominal obesity was independently associated with log-transformed CRP after controlling for other metabolic components. Among studies of overweight and obese children and adolescents, there was a different conclusion. Cizmecioglu et al. [23] reported no significant difference in hsCRP level between those with and without MetS. They concluded that inflammatory markers have no predictive value in the diagnosis of MetS. In contrast, Soriano-Guillen et al. [24] reported that obese children with MetS in Spain presented with higher level of hsCRP compared to those without MetS. After multivariate analysis, BMI, TG, and HDL-C were related to hsCRP. Oliveira et al. [21] reported that hsCRP was strongly related to the number of MetS components. They showed that excessive weight, hypertension, and hypertriglyceridemia were independently associated with hsCRP after adjusting for HOMA-IR in Brazilian overweight and obese youth. Meanwhile, Kitsios et al. [25] claimed that hsCRP was comparable in obese and overweight Greek children and adolescents with and without MetS. Nevertheless, subjects with NAFLD were shown to have significantly higher level of hsCRP compared to those without NAFLD. Suhett et al. [26] reported that increased hsCRP level was associated with all components of MetS in prepubescent Brazilian children aged 8–9 years (PASE Study). A study on Korean children and adolescents recently reported that hsCRP was associated with high BMI z-score, low HDL-C, and prediabetes [10].
This study found that prediabetes (HbA1c≥5.7%) was independently associated with hsCRP after adjusting for other metabolic factors. Studies of adults have shown that development of T2DM is highly associated with increased hsCRP, suggesting that low-grade chronic inflammation coexists with glucose intolerance and a compensatory increase in insulin secretion [27,28]. In a meta-analysis, the associations between inflammatory markers and risk of T2DM were described as robust [29]. Recently, Kato et al. [27] reported a significant association between elevated serum hsCRP level and prediabetes in middleaged Japanese adults. They showed that hsCRP level correlated significantly with impaired fasting glucose (IFG), impaired glucose tolerance (IGT), and elevated HbA1c level, all of which are indicators of prediabetes. In the Diabetes Remission Clinical Trial, significant longitudinal changes were found in markers of systemic inflammation with glycemic deterioration and changes in HOMA-IR in initially nondiabetic subjects followed for 7 years [28]. The failure to find an association between hsCRP and hyperglycemia in previous studies and ours might be due to the lower correlation of IFG with insulin resistance than that of IGT. [30,31]. An Italian research study found that normal glucose tolerance, IFG, IGT, and T2DM, but not IFG, were associated with elevated plasma IL-6 and hsCRP [32].
A significant advantage of this study is that it utilizes the NCEP-ATP III criteria based on a large nationally representative Asian population readily available to physicians. Also, NCEP-ATP III does not have to meet specific criteria, so the results are applicable even in lean MetS. However, we admit some limitations. First, the cross-sectional nature of this study prohibits conclusions regarding the existence of a causal relationship. However, it is well known that an elevated hsCRP level is a predictive factor for developing MetS, and there is potential to use hsCRP to identify higher-risk adolescents and prevent future adult disease. Second, there was no plasma insulin concentration data in the KNHANES 2016–2017. Thus, we could not adjust for IR, which weakened our results. Third, mild to moderate elevation of hsCRP might be partially influenced by subjects' acute infection, dietary habits, and exercise status, and these factors were not considered in the present study. Finally, caution must be exercised with interpretation of our findings because we defined prediabetes as HbA1c≥5.7% among those who had not previously been diagnosed with diabetes.
In conclusion, we confirmed that the association between the highest quartile of hsCRP was significantly related to increased risk for MetS in Korean children and adolescents using NCEPATP III criteria. This result confirms that hsCRP might be valuable in predicting MetS and prediabetes in Korean children and adolescents. However, further longitudinal investigations are needed to confirm whether the top quartile for hsCRP level increases MetS, T2DM, and CVD in Korean children and adolescents.
Ethical statement
The Research Ethics Committee of the Korea Centers for Disease Control approved the study protocol, and all participants or their parents signed a written informed consent form.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was partially supported by a grant from the Korea Institute of Radiological and Medical Sciences (KIRAMS), funded by the Ministry of Science and ICT (MSIT), Republic of Korea. (No.50541-2019).
Data availability
The data that support the findings of this study can be provided by the corresponding author upon reasonable request.
Author contribution
Conceptualization: KJH, LJS. Data curation: LJS. Formal analysis: KJH, LJS; Methodology: KJH, LJS. Writing - original draft preparation: KJH, LJS; Writing - review and editing: LJS.