Highlights
Transition care of T1D patients was a considerable challenge to pediatric endocrinologists. This national survey indicated many impediments for transition care in pediatric providers in Korea. Development of protocols for transition care is required to successful transition.
Introduction
Type 1 diabetes (T1D) is one of the most common chronic diseases in childhood [1,2]. Long-term management of the disease from childhood to adulthood is essential [3,4]. Along the course of disease management, there is a time to transfer from pediatric to adult healthcare system. The transition period corresponds to emerging adulthood, generally from the late teens to early twenties [5]. T1D patients in the transition period are associated with unfavorable health outcomes, including poor glycemic control, loss of follow-up, psychological problems, and increased acute and chronic complications [6-10]. Therefore, proper management in the transition period is critical for improving clinical outcomes in T1D patients.
For management of T1D patients in the transition period, the American Diabetes Association and other academic societies published a position statement in 2011, providing recommendations for transition care for pediatric providers and emerging adults with T1D [11]. In several guidelines and reviews, successful transition is an indispensable part of T1D care [12-15]. Although the Endocrine Society and other professional societies have developed several transition toolkits for T1D, it is uncertain whether these guidelines are well applied in clinical practice [16]. Moreover, there are no widely accepted guidelines or protocols for transition care in T1D patients.
To date, many studies have focused on issues related to patients/family of T1D patients [17-20], adult providers [21,22], and pediatric providers [23,24], especially in Western countries. However, studies on Korean patients are sparse [25] because the incidence of T1D in children and adolescents in Korea has been low, although increasing incidence has been observed [26,27]. Moreover, studies on transition care of T1D patients from the point of view of pediatric providers have not been carried out.
The aim of this study was to describe clinical practice characteristics and circumstances, investigate the reasons and impediments to T1D transition care, and identify clinical practice patterns of pediatric endocrinologists associated with transition care of patients with T1D, from the perspective of pediatric providers using a nationwide survey.
Materials and methods
1. Survey design
A structured questionnaire was designed based on practice circumstances of Korea and previous studies [22,24,28]. The questionnaire was comprised of three parts with 16 questions: (1) characteristics of responders including age, sex, and duration of practice as a pediatric endocrinologist; (2) practice circumstances including practice setting (primary, secondary, or tertiary center), number of patients with T1D, percentage of T1D patients aged 18 years or more, and composition of pediatric diabetes care team; and (3) process of transition such as reasons for transition, glycemic control at the time of transition, communication and feedback with adult endocrinologists, impediments to transition to adult clinic, and suggestions for improvement of transition care. The responses were in the form of "single most important answer" and "all relevant answers."
2. Data collection
Candidates for the survey were 143 pediatric endocrinologists in Korea who were registered in the Korean Society of Pediatric Endocrinology (KSPE) at the time of survey. Electronic survey was conducted using SurveyMonkey (Momentive Global Inc., Anaheim, CA, USA). An email embedded with the survey link was sent to all members of the KSPE on April 17, 2017. Data collected until April 30, 2017 were used for the analysis. Responses were anonymous, and there was no incentive to participate in the survey.
3. Statistical analysis
Data were analyzed using Stata 16.0 (StataCorp LP, College Station, TX, USA). Data were expressed as mean±standard deviation for continuous variables and number and percentage for categorical variables. Student t-tests and Fisher exact tests were used for comparison of continuous and categorical variables, respectively. A P-value of <0.05 was considered statistically significant.
Results
1. Characteristics and practice circumstances of responders
The survey response rate was 50.2% (n=72). Characteristics of responders are described in Table 1. Among responders, females were predominant (n=42, 58.3%). Practice duration as a pediatric endocrinologist was 13.0±8.9 years. Proportion of responders aged between 31 and 50 years was 75% (n=54). Fifty-one responders (70.8%) worked in tertiary centers. Number of patients with T1D varied, although 65.4% of responders followed ≤50 patients. Most responders (84.7%) had ≤25% of T1D patients aged ≥18 years.
Male respondents had a longer practice duration (15.8 years vs. 11.3 years, P=0.038) and more patients with T1D (P=0.041). There were no differences in sex and practice duration according to practice setting (P=0.867 and P=0.445, respectively). There was a tendency of increasing number of diabetes care team members (2.5 in primary, 3.1 in secondary, and 4.0 in tertiary center; P=0.007). The number of T1D patients was relatively high in tertiary centers (P=0.002).
2. Reasons and glycemic control in transition
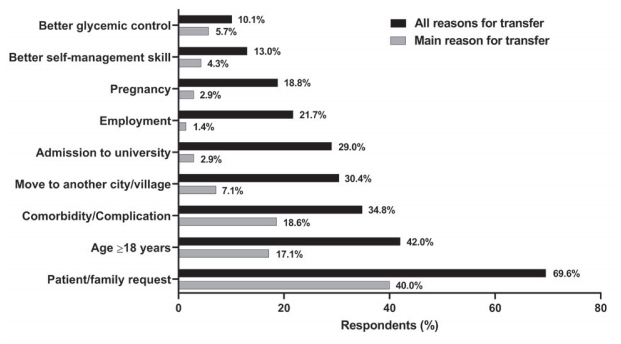
All relevant reasons for transfer to adult clinic were patient/family request (69.6%), age ≥18 years (42.0%), development of comorbidity or diabetes complications (34.8%), move to another city/village (30.4%), and admission to university (29.0%) (Fig. 1). The reasons for transfer were ranked as follows: patient/family request (40.0%), development of comorbidity or diabetes complications (18.6%), age ≥18 years (17.1%), move to another city/village (7.1%), and better glycemic control (5.7%).
With regard to glycemic control during transition, responses varied. T1D patients in transition were preferentially transferred to an adult clinic with very good glycemic control (glycosylated hemoglobin [HbA1c] < 7.0% [53 mmol/mol], 22.9%), good glycemic control (HbA1c 7.0%–8.5% [53–69 mmol/mol], 30.0%), poor glycemic control (HbA1c 8.6%–10.0% [70–86 mmol/mol], 12.9%), and very poor glycemic control (HbA1c > 10.0% [86 mmol/mol], 34.3%). There was no difference in glycemic control at transfer by sex and practice setting (all P>0.05).
3. Communication with adult endocrinologists
Pediatric endocrinologists in Korea communicated with adult endocrinologists via unstructured patient summary (68.6%), telephone or email (27.1%), overlap of pediatric and adult practice (12.9%), structured document (7.1%), or without any document or contact (12.9%) at the time of transition. After transfer, feedback from adult endocrinologists was by way of telephone (10.1%), letter or email (10.1%), or regular feedback (1.4%). However, 79.7% of respondents did not receive any feedback.
4. Impediments to transition care
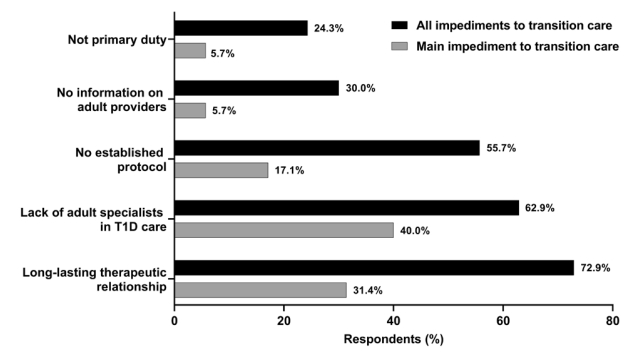
For pediatric endocrinologists, impediments to transition care were long-lasting therapeutic relationship with patient/family (72.9%), lack of adult specialists in T1D care (62.9%), no established protocol for transition care (55.7%), no information on adult providers (30.0%), and not having enough time because of low priority (24.3%) (Fig. 2). Forty percent of respondents considered lack of adult specialist in T1D care the most important impediment to transition care, followed by longlasting therapeutic relationship with patient/family (31.4%) and no established protocol for transition care (17.1%). There was no difference in sex or age by impediment (all P>0.05)
5. Suggestions for effective transition care
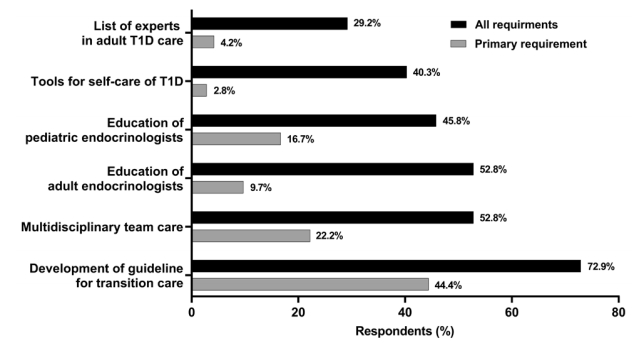
For effective transition care, respondents suggested the need for guidelines for transition care (72.9%), multidisciplinary team care with patient/family as well as pediatric and adult providers (52.8%), education of adult and pediatric providers (52.8% and 45.8%, respectively), development of tools for self-care evaluation of T1D (40.3%), and provision of a list of experts for adult T1D care (29.2%) (Fig. 3). Among them, development of guidelines for transition care (44.4%) was considered most important.
Discussion
To the best of our knowledge, the present study is the first on transition care from the perspective of pediatric providers in Korea and Asia, where the incidence of T1D is low. In this nationwide survey with a high response rate, pediatric endocrinologists in Korea indicated that patient/family request was the main reason for transfer to adult clinic, and lack of adult specialists in T1D care and long-lasting therapeutic relationship with patient/family were the main impediments to transition care. Pediatric providers in Korea mostly communicated with adult using unstructured documents, although almost 80% of the respondents did not receive any feedback after transfer. For effective transition care, pediatric endocrinologists in Korea considered development of guidelines for transition care as the most important factor.
The transition period in T1D patients is associated with unfavorable health outcome [6-10]. Transition indicates "planned and purposeful shift from a child- to adult-centered healthcare system." [29] Therefore, for successful transition and to reduce transition-related health problems, preparation for transition via participation of patient/family and pediatric and adult care providers is of paramount importance. Several guidelines have recommended that pediatric providers should start preparing for transition at least one year before transfer, although the appropriate age at transfer is unclear [11,14]. In the present study, two main reasons to embark on transition for pediatric endocrinologists in Korea were patient/family request and age ≥18 years, which were similar to another study [24]. Moreover, onethird of the respondents identified development of comorbidity or diabetes complications as reasons for transfer; pediatric providers can be unfamiliar with management of these complications. These responses imply that transition in Korea is a relatively passive but abruptly occurring process driven by outside circumstances rather than by diabetes team and patient/family engagement.
Diabetes self-management skills are key requirements for successful transition. A recent study showed that good executive functioning skills and balanced responsibility for diabetes management tasks between youth and parents were associated with better glycemic control around the transition period [30]. Therefore, during preparation for transition, education of T1D patients should focus on the gradual shift of care responsibility from the family to patients. However, in the present study, only 4.3% of respondents answered that better self-management skills were a primary reason for transfer. There is a wide gap between guidelines and real-world practice, and measures to fill this gap are necessary.
Impediments to transition care in this survey were termination of long-lasting therapeutic relationship with patient/family, lack of adult specialists in T1D care, and absence of established protocols. With regard to ending long-term relationship, no sex difference was observed in the present study, whereas female predominance was noted in another study [24]. T1D patients in Korea were managed by pediatric endocrinologists in hospitals rather than primary care physicians, because the incidence of T1D in childhood is very low and typically is diagnosed in hospitals. Therefore, pediatric patients with T1D tended to be transferred to adult endocrinologists in the same hospital, unless they were moving to another place or proceeding to university. However, due to a high prevalence of type 2 diabetes among adults in Korea, adult providers are mainly engaged in management of type 2 diabetes. As a result, it seems to be difficult to find adult specialists for T1D care in Korea. This might be the same in countries with a low incidence of T1D in childhood. Thus, this study highlights the challenges of low T1D incidence on transition care. Providing a list of adult experts for T1D care at the professional medical society level might be a countermeasure to tackle the lack of information.
Most pediatric endocrinologists in Korea communicated with adult counterparts via unstructured documents. However, adult care providers in the United States reported that patient records and summaries were an integral part of healthcare transition [22]. Therefore, development of structured documents with essential information for transition is necessary. Contrary to contact with adult endocrinologists around the time of transition in almost 90% of pediatric providers, approximately 80% of them did not receive any feedback from their adult counterparts after transfer. At transition, clinic attendance rate is associated with glycemic control [19,31]. To prevent missed attendance after transfer, mutual communication between pediatric and adult providers over the transition period might be required.
Korean pediatric endocrinologists considered development of guidelines as most important for an effective transition. In a Canadian study, a structured program for transition was helpful in improving clinical attendance and decreasing diabetes-associated distress [32]. Transition process varied by clinic [23]. Moreover, transition is influenced by psychosocial development of patient and family background. Therefore, culturally-sensitive and well-organized guidelines with detailed instructions are necessary. In addition, a multidisciplinary team approach including pediatric and adult providers is critical for preparation of a transition, which promotes diabetes self-care skills of patients and duties as emerging adults.
Many pediatric endocrinologists responded that education programs on transition care for both pediatric and adult care providers were necessary for effective transition. Training for transition care influenced several aspects such as smooth transition process, well-organized documentation, and less frequent return to the pediatric clinic [24]. In the present study, reception of transition education was not determined. However, such training is not common in Korea, and efforts to setup transition training programs are needed.
The present study had limitations. Almost half of the KSPE members did not respond to the survey request. However, the result of the study might reflect the situation in Korea since most doctors working in hospitals answered the survey. The survey also excluded adult endocrinologists, patients, and family members, who might have had different points of view on transition. However, this is the first study to evaluate the perspectives of pediatric endocrinologists on transition care in Korea and Asia, where the incidence of T1D is low.
In conclusion, our findings revealed that transition care of T1D patients was a considerable challenge to pediatric endocrinologists in Korea. This national survey indicated that development of a culturally sensitive protocol for transition care, multidisciplinary team approach, and education for pediatric and adult care providers are required for effective transition of T1D patients. Moreover, preparation for transition should be directed at improving self-management skills of emerging adults. In addition, unmet needs of adult care providers and patient/family should be investigated.