Mixed gonadal dysgenesis in 45,X Turner syndrome with SRY gene
Article information
Abstract
Turner syndrome is the most common chromosomal disorder in girls. Various phenotypic features show depending upon karyotype from normal female through ambiguous genitalia to male. Usually, Turner girls containing 45,X/46,XY mosaicism, or sex-determining region Y (SRY) gene may have mixed gonadal dysgenesis with various external sexual differentiation. We experienced a short statured 45,X Turner girl with normal external genitalia. Because SRY gene was positive, laparoscopic gonadectomy was performed. The dysgenetic gonads revealed bilateral ovotesticular tissues. The authors report a mixed gonadal dysgenesis case found in clinical 45,X Turner patient with positive SRY gene. Screening for SRY gene should be done even the karyotype is 45,X monosomy and external genitalia is normal.
Introduction
Mixed gonadal dysgenesis (MGD) is a disorder of the sexual differentiation characterized primarily by dysgenetic testicular tissue on one side and a streak gonad on the other. The clinical phenotype varies considerably and depends on the amount of secreted testosterone by fetal testis. Thus, the phenotype ranges from normal male through patients with ambiguous external genitalia to females1). MGD is heterogeneous in its etiology and that incomplete development of the testis can be due to an error in either testis determination or differentiation. Mutations in testis determining gene such as SRY are not generally found in this condition2). Dysgerminoma and clitoromegaly were reported as clinical evidence of Y chromosome material in 45,X Turner patients, whose SRY gene was detected in polymerase chain reaction-amplified DNA test3). Unrecognized Y-derived material is known to increase the risk of gonadal neoplasia, especially gonadoblastoma, therefore every effort should be paid for the detection of Y-derived material in Turner patients4)5)6).
In this report, authors report an MGD case found in clinical 45,X Turner patient with positive SRY gene.
Case report
Ten years and 3 month-old girl was brought to endocrine clinic for short stature. She was delivered uneventfully at 40 weeks of gestation with 3.2 kg. On exam, her height was 116 cm (<3th percentile), body weight was 19.3 kg(<3th percentile), breast was prepubertal. She had neither cubitus valgus deformity nor webbed neck. Knuckle sign was negative. Multiple freckles were found at back area. Audiometry, echocardiography, kidney ultrasonography were all normal. Her karyotyping revealed 45,X. After diagnosis of Turner syndrome, growth hormone had been given for the treatment of short stature, and estradiol replacement was started at 12.7 years of age. Because SRY gene was positive, she was scheduled to perform laparascopic gonadectomy at 14 years of age.
On pelvic laparoscopy, the uterus and both fallopian tubes looked normal, but both gonads looked streak in appearance (Fig. 1). Both adnexa were removed. On pathologic exam, salpinx was observed with dysgenetic gonad (Fig. 2). The dysgenetic gonad had stroma of whirling pattern with primordial follicles resembling ovarian stroma (Fig. 2A) and clusters of Leydig cells with ill-defined boundary (Fig. 2B). Vas deference was seen as tubular structures surrounded by fibromuscular stroma in certain part of stroma (Fig. 3), and seminiferous tubules were found with surrounding tunica albugina (Fig. 4A). Sertoli cells and spermatogonia were seen in the seminiferous tubules without spermatogenesis (Fig. 4B). On the other side of adnexa, dysgenetic ovarian stroma with whirling pattern, vas deference, and Leydig cell cluster were also observed. Pathologic findings were compatible to mixed gonadal dysgeneis.
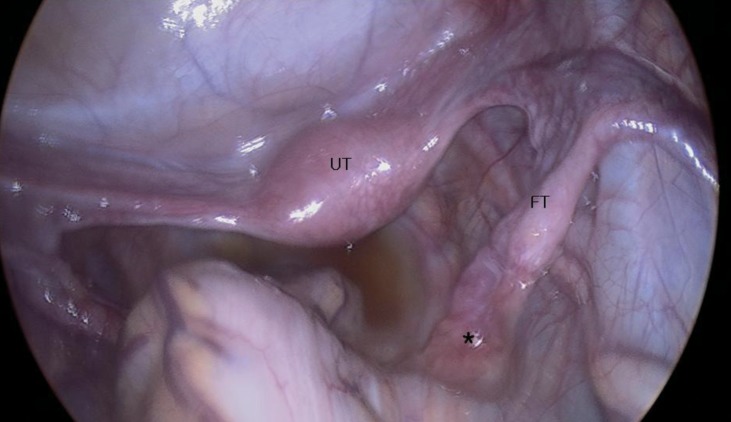
Laparoscopic finding of uterus and gonads. Laparosacopic view of normal uterus (UT), both fallopian tubes (FT), and streak gonad (*).
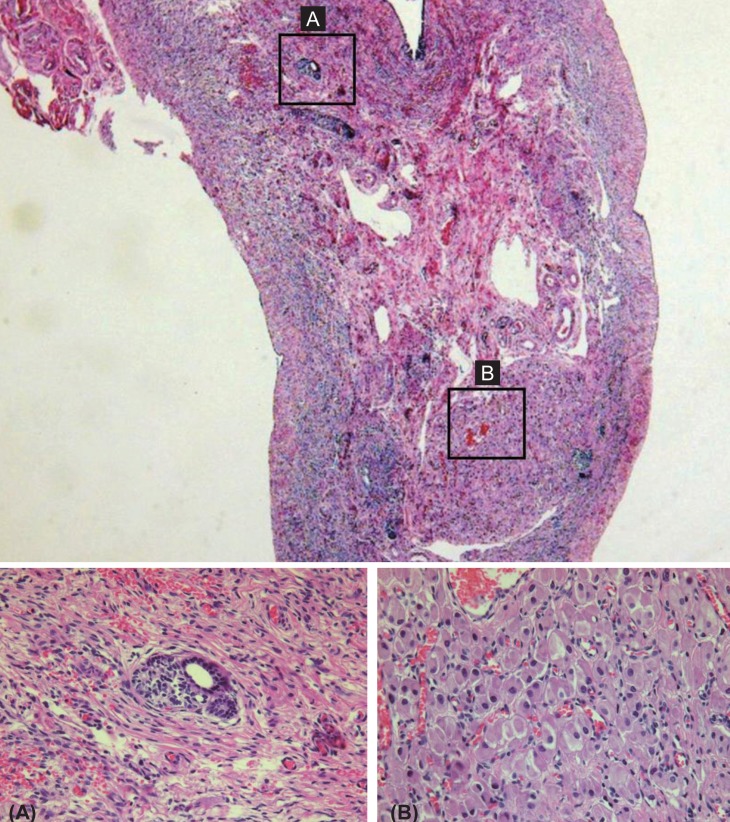
Dysgenetic gonad (H&E, ×40). (A) Ovarian stroma with whirling pattern and primordial follicles (H&E, ×200). (B) Clusters of Leydig cells with ill-defined boundery (H&E, ×400).
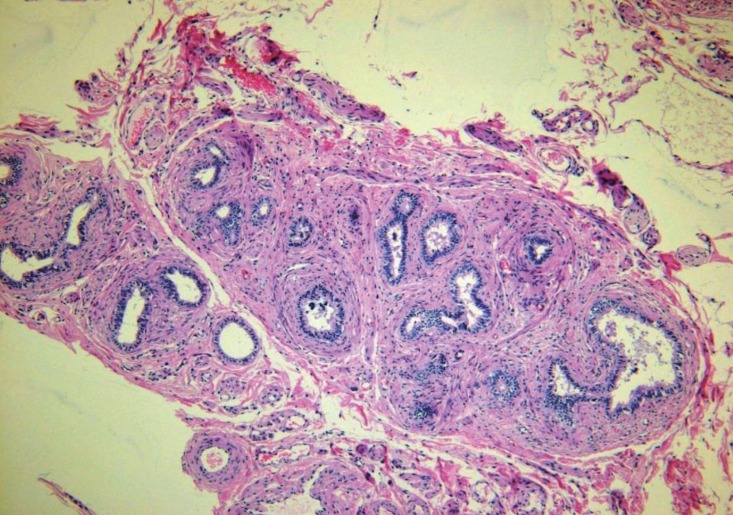
Vas deference as tubular structure surrounded by fibromuscular stroma (H&E, ×100). One part of dysgenetic gonad, tubular structure surrounded by thick fibromuscular stroma was confirmed to be vas deference consisting of simple cuboidal cells.
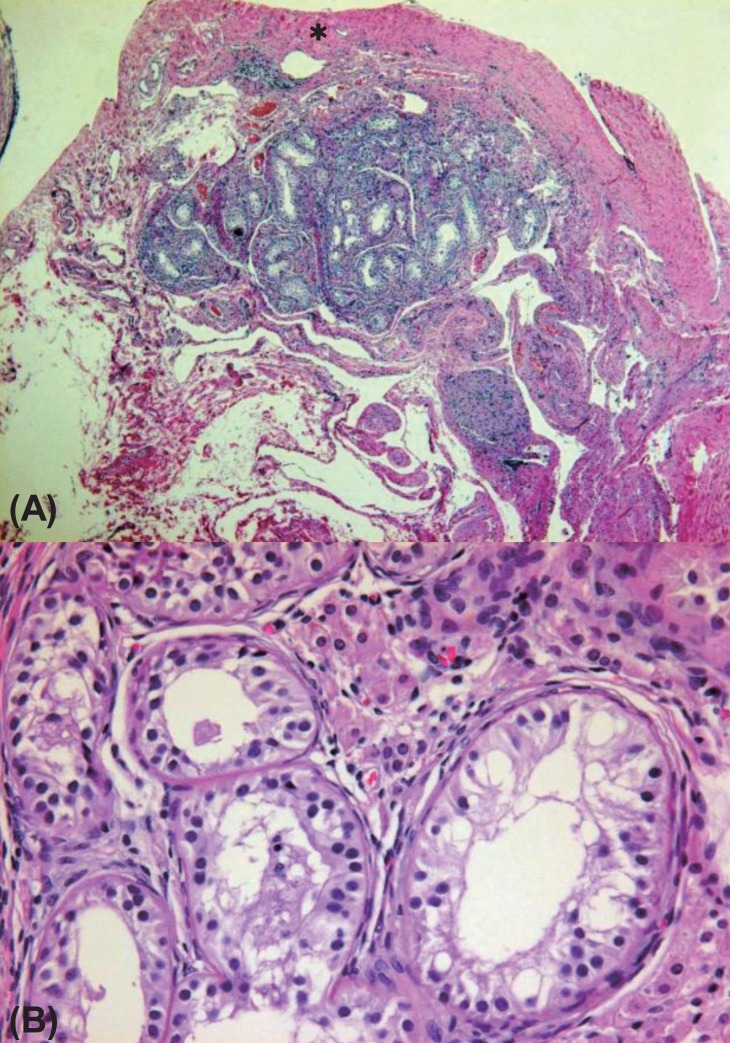
The other part of dysgenetic gonad, tubular structures were seen with surrounding thick fibrous tissue (*) tunica albugina (A). In high power view of the circle, tubular structures were confirmed to be typical seminiferous tubules with intermingling Leydig cells (B). (A) Seminiferous tubules surrounded by tunica albuginea (H&E, ×40). (B) Sertoli cells and spermatognoia (H&E, ×400).
Discussion
This case is genetically Turner syndrome with karyotype of 45,X, but pathologically mixed gonadal dysgeneis. The positive SRY gene is an evidence of unrecognized Y material which was not found in karyotyping.
Many studies demonstrated that 40%-60% of Turner patients were 45,X monosomy in blood lymphocytes, whereas the remaining patients had a structurally abnormal X- or Y-chromosome or were mosaics with a second cell line containing a normal or an abnormal sex chromosome7). Most MGD has mosaic 45,X/46,XY karyotype, but additional karyotypes including 45,X/47,XXY and 45,X/46,XY/47,XYY were reported1). Our case revealed 45,X in standard karyotyping, but positive SRY was the hallmark of the presence of cryptic Y material. Generally, standard 30-cell karyotyping is performed as recommended by the American College of Medical Genetics to identify at least 10% of mosaicism with 95% confidence8).
The clinical phenotype may range from almost normal female external genitalia with mild clitoromegaly, through ambiguous genitalia, to isolated hypospadias or normal male external genitalia. Usually the internal genital ducts align with the nature of ipsilateral gonad, with retention of a fallopian tube on the side adjacent to a severely dysgenetic streak gonad. The gonads are generally in combination of a well-formed testis on one side and a streak dysgenetic gonad on the contralateral side1). Our case showed no stigmata of Turner features, such as cubitus valgus deformity, shield chest, knuckle sign and webbed neck. Only she showed short stature and multiple freckles on the back area. And she also showed normal female external genitalia in spite of the dysgenetic gonads containing both ovarian and testicular tissues. This might be explained by the predominance of 45,X cell lines besides the presence of SRY preventing the development of testicular tissue9).
Usually, 45,X Turner syndrome had streaky gonad or immature ovary. But our patient showed combination ovarian tissue including primordial follicles and testicular tissue with spermatogonia and seminiferous tubules. This form of gonadal dysgenesis is typically observed in a mosaic 45,X/46,XY karyotype. Although our patient did not have Y chromosome, we could find SRY gene. Generally, 45,X Turner syndromes with no genital ambiguity, are not believed to be at risk for gonadoblastoma. Because ovaries of these patients rapidly degenerate into fibrous streaks with loss of oogonial germ cells10). Commonly gonadoblastoma arises from dysgenetic gonad. The risk for development of the tumor in Y-bearing dysgenetic gonad has been reported from 12.2% to 25%11)12). But several studies reported that gonadoblastoma occurred in patients with 45,X karyotype11)13). Canto et al.14) investigated the presence of Y-chromosome sequences in 107 Turner syndrome patients with a 45,X karyotype, and found them in 10 of these patients (9.3%). Two of 10 (20%) were confirmed gonadoblastoma after prophylactic gonadectomy. SRY gene is a single-exon gene (Yp11.3) that plays an important role as primary testisdetermining gene in normal testis development15). Bianco et al.16) observed that temporal exposure of dysgenetic gonad to Y-chromosome sequences, especially SRY, could lead to a clinical picture of hyperandrogenism in the gonadal microenvironment. It is supposed that SRY expression is reinforcing the role of this gene in the abnormal microenvironment of dysgenetic gonad, as the main determinant of neoplastic progression, providing the cell with equipment to survive and proliferation17). In conclusion, the detection of SRY gene in Turner syndrome is necessary to prevent the development of tumoral or nontumoral gonadal lesion, even if karyotyping using peripheral blood lymphocyte does not detect Y chromosme material.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.