Relationship between growth velocity and change of levels of insulin-like growth factor-1, insulin-like growth factor binding protein-3 and, IGFBP-3 promoter polymorphism during GnRH agonist treatment
Article information

Abstract
Purpose
This study aims to investigate the effect of gonadotropin-releasing hormone agonist (GnRHa) on the growth hormone (GH)-insulin-like growth factor-1 (IGF-1) axis and to evaluate whether -202 A/C IGF binding protein-3 (IGFBP-3) promoter polymorphism affects growth velocity in females with central precocious puberty (CPP) during treatment.
Methods
Data was collected from 97 females younger than 9 years, diagnosed with precocious puberty and treated with GnRHa for at least 1 year at Kangdong Sacred Heart Hospital from 2014 to 2015. Their body height, weight, change in height standard deviation score (∆SDS), serum IGF-1, serum IGFBP-3, bone age, and -202 A/C IGFBP-3 promoter polymorphism were measured before and after GnRHa treatment. The interrelationships between the variables were calculated.
Results
During treatment, height SDS, IGF-1 SDS, IGFBP-3 SDS, and IGF-1/IGFBP-3 ratio significantly decreased. A significant correlation was observed between ∆IGF-1 SDS and ∆height SDS (r=0.405, P<0.001). The presence of the C allele was significantly correlated with IGF-1 SDS after treatment (P=0.049) and with IGFBP-3 SDS before and after treatment (P=0.012 and P=0.001), but not with ∆IGF-1 SDS, ∆IGFBP-3 SDS, ∆IGF-1/IGFBP-3 ratio, or ∆height SDS.
Conclusions
Growth velocity during GnRHa treatment is related to ∆IGF-1 SDS, indicating the apparent impact of GnRHa on the GH-IGF-1 axis. The -202 A/C IGFBP-3 promoter polymorphism does not affect the growth velocity of GnRHa in CPP girls.
Introduction
When females and males younger than 8 and 9 years, respectively, undergo secondary sexual changes caused by stimulation of the hypothalamic-pituitary-gonadal axis, they are diagnosed with central precocious puberty (CPP) [1]. A recent study reported an increasing number of CPP patients in South Korea from 2008 to 2014 [2]. Concerns regarding the negative effects of CPP are increasing, one of which includes reduced stature caused by accelerated early growth and bone maturation [3].
Gonadotropin-releasing hormone agonist (GnRHa) is the treatment of choice in CPP patients because it increases final adult height by reducing progression of bone age (BA) and extending the duration of growth [4]. GnRHa induces downregulation of the hormonal axis and decreases the production of luteinizing hormone (LH) and follicle-stimulating hormone, resulting in gonadal suppression. These sex hormones are responsible for early bone maturation and pubertal growth spurts. Therefore, gonadal suppression delays bone maturation and growth velocity to those of prepuberty levels [5].
Multiple factors such as initial chronological age (CA), initial height, target height, and BA advancement affect the treatment response and final height [6-8]. GnRHa treatment increases serum growth hormone-binding protein concentration and decreases serum IGF-I and IGFBP-3 concentrations [9]. However, predicting final height remains a challenge due to the variable factors affecting the treatment outcome and the course of precocious puberty.
Other genetic components are presumed to influence the competence of GnRHa. Specifically, -202 A/C IGFBP-3 promoter polymorphism is associated with increased IGFBP-3 level and growth velocity during growth hormone (GH) treatment for prepubertal GH deficiency [10,11]. Another study revealed the effect of -202 A/C IGFBP-3 promoter polymorphism on the physical development of Korean females. However, its effect was unclear [12].
The present study was performed to clarify the effect of GnRHa on the GH-IGF-1 axis and to evaluate the predictive role of -202 A/C IGFBP-3 promoter polymorphism on growth velocity during GnRHa administration in females diagnosed with CPP.
Materials and methods
1. Patients
This study enrolled 97 young female subjects between the ages of 6 and 8 years who were diagnosed with CPP and administered GnRHa at Kangdong Sacred Heart Hospital, Seoul, Korea, from January 2014 to January 2015. The subjects were diagnosed with CPP when they presented with breast budding above Tanner stage B2 before 8 years of CA, revealed BA advancement of more than one year compared to CA, and had 5 IU/L or greater peak LH level after the gonadotropin releasing hormone stimulation test. In total, 22 subjects who were diagnosed with hypothyroidism, GH deficiency, or congenital adrenal hyperplasia or who underwent previous GH treatment or were born small for gestational age were excluded. GnRHa was injected every 4 weeks. Children weighing more than 30 kg were injected with 3.75 mg of GnRHa, compared to 2.5 mg for those below 30 kg.
2. Measurements
Body height and weight, serum IGF-1 and IGFBP-3 concentrations, and the BA of patients were measured before and one year after GnRHa treatment. A Harpenden Stadiometer (Holtain Ltd., Pembs. UK) was used to approximate height to the closest 0.1. Thereafter, body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Midparental height (MPH) was calculated by adding the height of the parents, subtracting 13, and dividing by 2. An IGF-1-D-RIA-CT kit (Biosource, Nivelles, Belgium) was utilized to measure serum IGF-1 concentration through the radioimmune method, whereas an immunoradiometric assay with Immunotech IRMA IGFBP-3 kit (Immunotech, Marseile, France) was used to evaluate the serum IGFBP-3 concentration. BA was based on left hand anteroposterior radiographs, and the measurements were performed in accordance with the Greulich and Pyle Atlas [13].
3. Molecular study
Genomic DNA was extracted from patient blood samples. The target IGFBP-3 gene containing -202 A/C polymorphic sites of 459 base pairs (bp) at the promoter region was amplified using corresponding sense and antisense primers. The polymerase chain reaction (PCR) product was sheared using the Alw21I restriction enzyme (Thermo Scientific, Waltham, MA, USA) to verify the allele types through restriction fragment length polymorphism and agarose gel electrophoresis. The PCR product was digested into 242-bp and 162-bp fragments containing an A allele and into 288-bp and 162-bp fragments when a C allele was present [14].
4. Statistical analysis
The definition of age-adjusted height velocity was established according to the difference between initial height SDS and final height SDS to minimize the confounding effect of age. Height SDS was calculated using Cole's modified least mean squares (LMS) algorithm [15]. The LMS values were provided by the 2007 version of Korean National Growth Charts for Children and Adolescents [16]. For IGF-I and IGFBP-3 SDSs, the LevenbergMarquardt algorithm was used to estimate the parameters from percentile values in Korean females [16,17]. Changes of IGF-1 and IGFBP-3 SDSs after GnRHa treatment were calculated and expressed as ∆SDS. The molar ratio of IGF-1 and IGFBP-3 was calculated, and the ratio of IGF-1/IGFBP-3 after treatment over the initial value was calculated and expressed as ∆IGF-1/IGFBP-3 ratio.
The mean, SDS, minimum, and maximum values of the continuous data were obtained by descriptive statistics and compared for statistical significance using paired t-test before and after treatment. Pearson correlation analysis evaluated the association between ∆height SDS and parameters of BMI, initial height SDS, MPH, BA advancement, and ∆IGF-1 SDS, ∆IGFBP-3 SDS, and ∆IGF-1/IGFBP-3 ratio. Univariate and multivariate regression analyses were performed to investigate the effects of ∆IGF-1 SDS, ∆IGFBP-3 SDS, and ∆IGF-1/IGFBP-3 ratio on ∆Height SDS. All covariates associated with the height velocity from the Pearson correlation analysis adjusted for initial height SDS, ∆IGF-1 SDS, ∆IGFBP-3 SDS, and ∆IGF-1/IGFBP-3 ratio.
The target patients were arranged into 2 subgroups based on the allele of -202 A/C IGFBP-3 promoter polymorphism. Independent t-test was performed between the 2 subgroups for SDS values of height, IGF-1, IGFBP-3, and IGF-1/IGFBP-3 before and after treatment. ∆IGF-1 SDS, ∆IGFBP-3 SDS, ∆IGF-1/IGFBP-3 ratio, and ∆height SDS were compared between the 2 subgroups. The differences of IGF-1 SDS and IGFBP-3 SDS before and after GnRHa treatment within the subgroups were confirmed by paired t-test.
All statistical analyses were performed with IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA). A value of P<0.05 was considered statistically significant.
Results
Mean values of CA, BA, MPH, height SDS, and BMI before treatment were 8.5±0.5 years, 10.5±0.6 years, 160.0±3.2 cm, 1.2±0.8, and 18.2±2.4, respectively. The SDSs for serum IGF-1 and IGFBP-3 concentrations were 0.8±1.0 and 3.3±1.1, respectively, and the IGF-1/IGFBP-3 ratio was 60.7±16.3. Subsequently, the mean BA value after one year of treatment was 10.9±0.6 years. The difference between BA and CA was significantly reduced from 2.0±0.6 to 1.3±0.6 (P<0.001) and the height SDS to 1.1±0.8 (P<0.001) after GnRHa. SDSs of serum IGF-1 and IGFBP-3 concentrations significantly decreased to 0.5±0.9 (P<0.001) and 2.3±0.9 (P<0.001), respectively. However, there was no significant change in IGF-1/IGFBP-3 ratio after treatment (P=0.887) (Table 1).

Characteristics of the 97 girls treated with GnRHa
∆IGF-1 SDS (r=0.405, P<0.001), ∆IGFBP-3 SDS (r=0.228, P=0.025), and ∆serum IGF-1/IGFBP-3 ratio (r=0.204, P=0.045) showed significant positive correlations with ∆height SDS. On the other hand, initial height SDS was negatively correlated with ∆height SDS (r=-0.307, P=0.002). Correlation analysis between ∆Height SDS, BMI, MPH, and BA advancement showed no statistical significance (Table 2). Only ∆IGF-1 SDS was significantly related to ∆height SDS on multivariate regression analysis after adjusting for covariates of ∆IGF-1 SDS, ∆IGFBP-3 SDS, ∆IGF-1/IGFBP-3 ratio, and initial height SDS (β=0.110, P≤0.001) (Table 3).
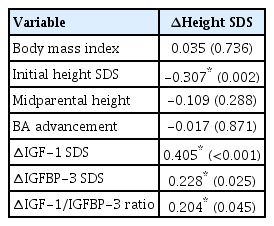
Pearson correlation analysis
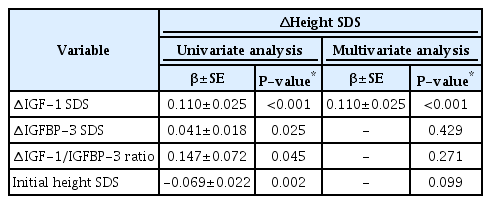
Univariate and multivariate regression model to find factors associated with Δheight SDS
According to the -202 A/C IGFBP-3 promoter polymorphism analyses, 72 AA genotypes (74.2%), 22 AC genotypes (22.7%), and 3 CC genotypes (3.1%) were present. The C allele frequency accounted for 14.4% of the study population. These genotypes were divided into 2 subgroups based on C allele presence. No significant difference was observed in IGF-1 SDS before treatment between the 2 subgroups (P=0.421). However, the group with the C allele exhibited notably lower IGF-1 SDS after treatment (P=0.049). IGFBP-3 SDS was lower in the C allele groups both before and after GnRHa treatment (P=0.012 and P=0.001, respectively). Height SDS IGF-1/IGFBP-3 ratio, ∆IGF-1 SDS, ∆IGFBP-3 SDS, ∆IGF-1/IGFBP-3 ratio, and ∆height SDS between the 2 subgroups exhibited no significant differences before and after treatment (Supplementary Table 1). There were significant changes of IGF-1 SDS after GnRHa treatment within both subgroups (P=0.005 and P<0.001, respectively) (Fig. 1A). IGFBP-3 SDS also significantly decreased in both subgroups (P<0.001 and P<0.001, respectively) (Fig. 1B).
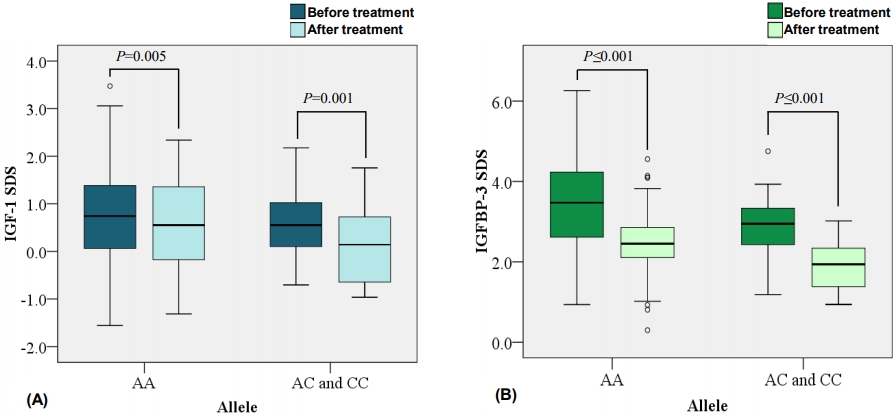
The graphs resemble the differences of IGF-1 SDS (A) and IGFBP-3 SDS (B) before and after GnRHa treatment within the two allele subgroups. GnRHa, gonadotropin-releasing hormone agonist; SDS, standard deviation score; IGF-1, insulin like growth factor 1; IGFBP-3, insulin-like growth factor binding protein 3.
Discussion
The GH-IGF axis directly or indirectly influences skeletal development, especially during puberty. However, the mechanism of IGF-1 or IGFBP-3 action during puberty and how the hormones interact with each other remain unclear. Juul et al. [18] discovered that the increase of free IGF-1 in puberty is not directly influenced by IGFBP-3 proteolysis. Verrotti et al. [19] compared the IGF-1 and IGFBP-3 concentrations between the 2 treatment regimens of GnRHa with or without cyproterone acetate and concluded that IGF-1 and IGFBP-3 are regulated by different metabolic pathways.
Despite continuous attempts to effectively understand GnRHa action upon the GH-IGF-1 axis, studies have reported disparate results. Numerous previous studies have presented trivial changes in serum IGF-1 or IGFBP-3 level during GnRHa treatment in CPP patients [20-23], in contrast to other studies where IGF-1 concentration decreased [9,18]. The present study aimed for a well-controlled project design to revise the GnRHa effect on the GH-IGF-1 axis and its relationship with height change. IGF-1 SDS and IGFBP-3 SDS decreased after 1 year of GnRHa treatment. However, after analyzing ∆IGF-1 SDS, ∆IGFBP-3 SDS, and ∆IGF-1/IGFBP-3 ratio with ∆Height SDS, only ∆IGF-1 SDS was significantly related. This result supports that IGF-1 plays a major role in pubertal height gain, and that a decrease in IGF-1 during GnRHa treatment restores the growth velocity to that before puberty. Among the numerous characteristics that increase final adult height in treated CPP patients, other than the GH-IFG-1 axis [6-8], we reevaluated BA advancement, initial height SDS, BMI, and MPH to determine whether they influenced growth velocity during GnRHa treatment. However, none were statistically associated with ∆Height SDS, suggesting that it is inappropriate to predict final adult height in CPP females based on BA, body figure, or parental height.
The -202 A/C IGFBP-3 promoter polymorphism has been suggested to be a potential genetic determinant that alters the GH-IGF-1 axis. Studies have reported that the presence of the C allele genotype is associated with low serum IGFBP level [24-26]. Since IGFBP has a role in pubertal growth, there is a potential for -202 A/C IGFBP-3 promoter polymorphism to affect growth velocity and final adult height. Nevertheless, it was difficult to confirm a concrete correlation due to the discrete results. According to Miletta et al. [27] the IGFBP-3 genotype had no effect on final height after GH treatment in severe GHD patients. In contrast, Costalonga et al. [10] implied that the -202 A allele polymorphism of the IGFBP-3 promoter region was associated with not only higher IGFBP-3 levels, but also increased growth during recombinant human GH treatment in prepubertal GHD children.
This study focused on the effect of the -202 A/C IGFBP-3 promoter polymorphism on the GH-IGF-1 axis as well as the growth velocity in CPP females undergoing GnRHa treatment for at least 1 year. We compared SDS of IGF-1 and IGFBP-3 between the 2 subgroups before and after GnRHa treatment. The results showed that IGF-1 SDS was not statistically different before treatment, but the group with the C allele after treatment demonstrated lower IGF-1 SDS than the AA subgroup. The IGFBP-3 SDS was lower in the C allele subgroup both before and after GnRHa treatment. However, change of IGF-1 SDS, IGFBP-3 SDS, or IGF-1/IGFBP-3 during treatment exhibited no significant difference between the 2 subgroups. Divergence of age-adjusted height velocity between the 2 allele groups was trivial. The effect of GnRHa on IGF-1 SDS or IGFBP-3 SDS was noted in both subgroups, regardless of allele. This suggests that -202 A/C IGFBP-3 promoter polymorphism does not significantly affect the therapeutic effect of GnRHa in CPP females.
Our study was carefully designed with a uniform diagnosis and treatment protocol in which GnRHa was administered every 4 weeks to all enrolled CPP patients. Target patients with the C allele alone could not substantially contribute to a definitive conclusion due to the small number. Therefore, children with CC and AC genotypes of -202 A/C IGFBP-3 promoter polymorphism were pooled into a single subgroup. This is due to a racial characteristic that the Korean population has a higher proportion of the A allele compared to other populations [12,25,28]. Another limitation of our study is that free IGF-1 level was estimated using the IGF-1/IGFBP-3 ratio. This estimation, however, is based on a previous study conducted by Juul et al. [18] showing that free IGF-1 concentration significantly correlates with the molar ratio of IGF-1 and IGFBP-3.
In conclusion, growth velocity during GnRHa treatment is related to ∆IGF-1 SDS, and GnRHa seems to have an impact on the GH-IGF-1 axis. The C allele in the -202 A/C IGFBP-3 promoter regions was not associated with the growth rate during GnRHa treatment in CPP girls and did not affect the reduction of IGF-1 SDS or IGFBP-3 SDS during treatment.
Notes
Ethical statement
The study was approved by the Institutional Review Board of Kangdong Sacred Heart Hospital (approval number: 2014-02-003). Informed consent was obtained from the parents or legal guardians of the children.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was financially supported by a research grant from the Investigator-Initiated Trials program of Ferring Pharmaceuticals. Opinions expressed in this paper are those of the authors and do not necessarily represent those of Ferring Pharmaceuticals. The authors would thank Ferring Pharmaceuticals for supporting this research.
Supplementary Materials
Supplementar y Table 1 can be found via https://doi.org/10.6065/apem.2040020.010