Age of menarche and near adult height after long-term gonadotropin-releasing hormone agonist treatment in girls with central precocious puberty
Article information
Abstract
Purpose
Gonadotropin-releasing hormone agonist (GnRHa) is known for improving final adult height in patients with central precocious puberty (CPP). This study aimed to investigate the age of menarche and near adult height in girls with CPP who had been treated with GnRHa.
Methods
In this retrospective study, we reviewed the medical records of 71 Korean girls with CPP who had started menarche or reached over 13 years of bone age after long-term GnRHa treatment. We estimated near adult height using the Bayley-Pinneau method and identified the age of menarche in girls with CPP.
Results
Mean chronological and bone age at menarche were 11.9±0.7 and 12.8±0.4 years, respectively. The period between menarche and the end of treatment was 14.0±5.6 months. Posttreatment near adult height was 163.8±4.7 cm, which was significantly greater than pretreatment predicted adult height (158.7±4.1 cm).
Conclusion
GnRHa treatment in girls with CPP could improve final adult height and made the age of menarche close to that of the general population.
Introduction
Central precocious puberty (CPP) is defined as the onset of secondary sexual characteristics before the age of 8 years for girls and 9 years for boys, which is usually due to the premature activation of the hypothalamic-pituitary-ovarian axis (H-P-G axis)1). Early diagnosis and treatment of CPP is important to improve final height because CPP can cause early epiphyseal maturation with compromised final height as well as psychological stress2,3).
Gonadotropin-releasing hormone agonist (GnRHa) is constantly combined to gonadotropin-releasing hormone receptor of pituitary gland, which is known as a safe and effective treatment for controlling premature H-P-G axis activation. Several studies reported that GnRHa treatment in CPP improved predicted adult height (PAH) in the target height range4,5,6,7,8). However, there were a few reports about the age of menarche or final adult height after GnRHa treatment because of difficulties with continuous follow-up observation after the end of treatment.
The aim of this study was to investigate the age of menarche and near adult height in girls with CPP who had been treated with GnRHa.
Materials and methods
1. Subjects
In this retrospective study, we reviewed the medical records of 71 Korean girls with CPP, from March 2003 to February 2011 at a pediatric endocrinology clinic of Korea University Hospital. All subjects were treated with GnRHa and they had showed menarche or reached over 13 years of bone age (BA) after GnRHa treatment.
CPP was diagnosed by the appearance of secondary sexual maturation under the age of 8 years, BA advancement, and a pubertal peak luteinizing hormone level≥5 IU/L. To exclude other forms of precocious puberty, further laboratory and imaging studies were performed based on clinical judgment. CPP patients with identified etiology, such as brain tumor or cranial irradiation, were excluded.
2. Methods
All patients were injected with leuprolide acetate, 75-100 µg/kg every 4 weeks and height, weight, and degree of pubertal development were checked. After GnRHa treatment, the patients regularly followed every 3 months to observe the changes of height, sexual maturity and menarche.
Their BAs were evaluated every six months by taking the left hand x-ray. BA was assessed by two pediatric endocrinologists using the Greulich-Pyle method, and PAH was estimated using the Bayley-Pinneau method9).
For the comparison with auxological parameters at the onset of GnRHa treatment, subjects were divided into three groups: <8 years, 8-9 years, and 9-10 years.
3. Statistical analyses
Statistical analyses were performed using IBM SPSS version 20.0 (IBM Co., Armonk, NY, USA). Multiple linear regression analysis was used for measuring the association of multiple clinical factors on PAH. The comparison among three groups mentioned before was applied using analysis of variance. All data were expressed as means±standard deviation. The P-value of <0.05 was considered as statistically significant.
Results
1. Comparison of clinical and auxological characteristics of subjects between at the start of the treatment and at the last visit after the treatment
At the start of GnRHa treatment, the mean chronological age (CA) and BA were 8.5±0.7 and 10.4±0.8 years, respectively. The difference between BA and CA was 1.9±1.2 years. At the last visit after treatment, the mean CA and BA was 12.3±0.8 and 13.5±0.6 years. The difference between BA and CA decreased to 1.2±1.0 years. The mean mid parent height (MPH) was 161.6±3.6 cm. The near adult height at the last visit was taller than pretreatment PAH (163.8±4.7 cm vs. 158.7±4.1 cm). Mean height standard deviation score (SDS) for CA and BA showed no significant differences between at the start of the treatment and at the last visit after the treatment (Table 1).
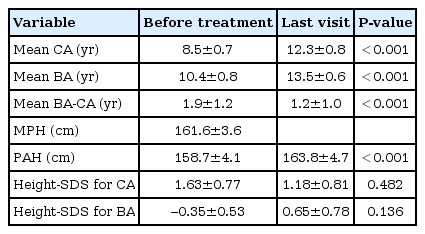
Auxological data of subjects (n=71)
2. Duration of the treatment and the age of menarche
The mean duration of GnRHa treatment was 27.9±9.0 months. The time interval from the end of the treatment to menarche was 14.0±5.6 months. The mean CA and BA at menarche of 52 girls who started the menarche were 11.9±0.7 and 12.8±0.4 years, respectively (Table 2). The time interval of menarche after the end of treatment was not correlated with any other factors (duration of treatment, CA at the end of GnRHa, BA at the end of GnRHa, height at the end of GnRHa) by using simple linear regression analysis.

Time of menarche and duration of treatment (n=52)
3. Comparison of PAH according to the age at the onset of GnRHa treatment
Subjects were divided into three groups to observe the difference of PAH and the age of menarche according to the age at onset of GnRHa treatment: <8 years, 8-9 years, 9-10 years. There were no significant differences in the period between menarche and the end of treatment among the three groups. The trend showed that the more treatment is delayed the less PAH increases: 5.9±3.7 cm, 4.8±2.9 cm, 3.8±2.3 cm, respectively. However, there was no significant difference among the three groups (P=0.095) (Table 3).
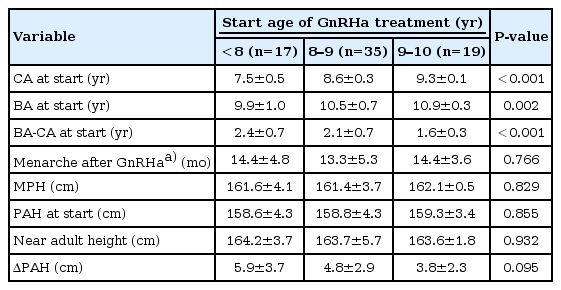
Change in difference of PAH and time of menarche in according to start age of GnRHa treatment
4. The correlation between near adult height and other auxological factors
Univariate analysis using simple linear regression was performed for correlation between near adult height and other auxological factors. Near adult height was significantly correlated with MPH (P<0.001), BA-CA at start (P=0.024), PAH at start (P<0.001), PAH after treatment (P<0.001), height SDS for BA at onset of treatment (P<0.001), and height SDS for BA after treatment (P<0.001). Near adult height was not correlated with duration of treatment, CA or BA at start. After multicollinearity checking among explanatory variables (MPH, BA-CA at start, PAH at start, PAH after treatment, height SDS for BA at start, height SDS for BA after GnRHa), a multivariate analysis using multiple linear regression revealed MPH and PAH after treatment were independently correlated with near adult height (Table 4).
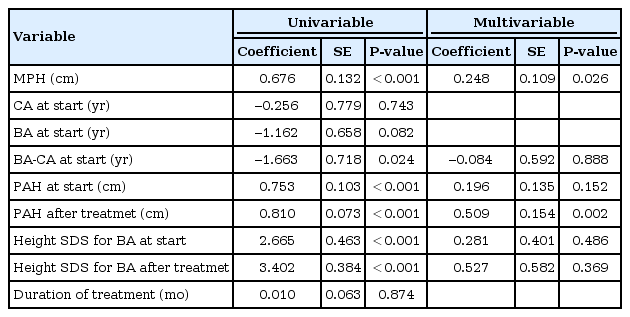
The correlation between near adult height and multiple factors
Discussion
This study is about the comparison of pretreatment PAH and adult height after the GnRHa treatment and investigation of actual age of menarche. The results of this study showed that long-term GnRHa treatment improved final height in girls with CPP. We also found that the age of menarche in girls treated with GnRHa was comparable to that of the general population10).
CPP in girls is defined as the appearance of secondary sex characteristics before the age of 8 years due to premature activation of the H-P-G axis. Idiopathic CPP excludes precocious puberty caused by specific conditions, for example, structural brain lesions, thyroid disorders, diabetes, chronic renal failure, and congenital adrenal hyperplasia. The secretion of growth hormone and insulin-like growth factor-I is augmented by sex hormone stimulation. The rate of growth and bone maturation is also rapidly increased. That leads to short final adult height.
After GnRHa treatment, the patients need follow up to observe the changes of height and sexual maturity. However, there are a few reports regarding the actual age of menarche and final adult height because most patients rarely attend the follow up clinic continuously after GnRHa treatment. In previous studies, to evaluate the effect of treatment intervention, growth velocity or PAH estimation in the short term were generally used4,5). Some author reported on final height of CPP girls too small selected groups8). In this study, we investigated actual age of menarche and measured near adult height with long-term follow-up after GnRHa treatment.
A recent survey showed the age of menarche in Korea is getting younger from 16 years in 1920s to 12.6 years in 1990s10,11). Untreated patients with precocious puberty encountered menarche earlier than the general population. In this study, the mean CA at menarche was 11.9 years and BA was 12.8 years. The age of menarche was comparable to the general population due to the treatment. The time interval from the end of the treatment to menarche was 14.0±5.6 months, which was similar to previous studies12).
According to some reports, adult height after the GnRHa treatment increases although there are some different effects in number13,14,15,16). In our study, pretreatment mean BA was 1.9 years advanced compare to mean CA. However, after treatment, the differences decreased to 1.0 years, which means it works well in inhibiting bone maturity. Pretreatment PAH was 158.7 cm, which was only 2.9 cm shorter than MPH of 161.6 cm, which is the target height in this study. The Bayley-Pinneau method has been used for PAH, although it has been criticized for the methods used to predicted height, as the results were taller than actual adult height17). In addition, for younger children, PAH is taller than actual height18,19). At the last follow-up after the treatment, we considered that girls reached near adult height at around 13.5 years of BA. Near adult height was 5.1 cm taller than pretreatment PAH. Consequently, this study verified that GnRHa has a positive effect on adult height.
Patients were divided into three groups, <8 years, 8-9 years, 9-10 years, to investigate change of PAH by onset age of treatment. However, there was no distinction among three groups. This result differs from a previous report20). It may have been similar if we had investigated a larger number of girls or divided the groups according to age like the previous study. On the other hand, effect on final adult height is not significant if GnRHa treatment begins before 10 years old.
In the previous study, there was a negative correlation between final height and CA or BA at onset of treatment21). Our study also showed negative correlation between near adult height and BA-CA at start (P=0.024). But there was no significant correlation between near adult height and CA at start or BA at start. This may be due to the relatively small sample size. Multiple regression analysis revealed that there were no significant correlation between near adult height an BA-CA at start. Significant variables were only MPH and PAH after treatment.
Through long-term follow-up, we investigated the near adult height of girls with CPP who reached over 13 years of BA after GnRHa treatment, but this was not the actual final adult height. In a recent study, it was generally known that a girl's growth velocity rapidly decreases after age 13 and then grows only a few centimeters to reach final height22). Another possible limitation of this study was that the sample scale was relatively small.
In conclusion, long-term GnRHa treatment could improve final height in girls with CPP, and the age of menarche of girls with GnRHa becomes close to that of the general population. We recommend continuous follow-up of CPP girls after GnRHa treatment to identify the occurrence of menarche and investigate long-term implications for general health status including final adult height.
Notes
No potential conflict of interest relevant to this article was reported.