Relationship of age at menarche on anthropometric index and menstrual irregularity in late adolescent girls in Seoul
Article information
Abstract
Purpose
To examine the relationship between menarcheal age and anthropometric indices and menstrual irregularity in late adolescent girls in Seoul.
Methods
We surveyed 4,218 fertile adolescent girls between the ages of 16 and 18 years to determine their anthropometric indices and menarcheal age. Measurements were taken from June 2008 to October 2009 at seven girl's high schools in Seoul, Korea. Participants were offered self-report questionnaire as a survey tool that included questions on anthropometric indices (height, weight, waist circumference), menarcheal age, menstrual pattern, frequency of menstruation per year.
Results
The participants were categorized into three groups based on menarcheal age: early menarche group (younger than 2 standard deviations [SD]), mid menarche group (within ±2 SD), late menarche group (older than 2 SD). The mean age of early menarche group was 9.9±0.2 years, mid menarche group 12.5±0.9 years, late menarche group 15.1±0.3 years (P < 0.001). Heights were recorded as 160.4±5.2 cm, 161.8±4.9 cm, 162.3±4.7 cm in early, mid, and late menarche group, respectively (P = 0.001). Body mass index (BMI) and waist circumference significantly were lager in early menarche group than mid and late menarche ones (P < 0.001). The menarcheal age had a positive correlation with height and negative correlations with weight, BMI, waist circumference (P < 0.001). The prevalence of oligomenorrhea was more frequent in late menarche group than early and mid menarche group.
Conclusion
The menarcheal age have positive relationship with height and inverse relationship with BMI and waist circumference in late adolescent girls in Seoul. Late menarcheal girls are disposed to have menstrual irregularity compared to early menarcheal girls.
Introduction
Menarche is an essential event of sexual maturation and a major indicator of female maturity1). The mean menarcheal age is known to be affected by various parameters including body fat accumulation, nutrition, environmental conditions, socio-economic status, genetic cause, and exposure to endo-neurocrine disruptors1-4).
The menarche age showed recently downward tendency worldwide, with a diminution of 2-3 months per decade in western countries and the United States1,5-8). In Korea, menarcheal age declined from 17 to 15 years in the 1960s, to 14 years in the 1980s, and to 13 years in the 1990s9).
Early menarcheal age is known to be a critical impact for many health disorders10-13). Girls who experienced early menarche tend to be more obese in adulthood life14). It has been suggested that girls who undergo menarche early may have a longer period of a positive energy balance or many endo-neurocrine components affect the speed of sexual maturation and body fat accumulation14). Thus, early menarcheal age causes precocious shutdown of the plates, and girls who undergo menarche early have a shorter final adult height compared to late menarche groups15).
The mean menarche age was found to gradually decline, while the age at beginning of regular menstrual cycle increased steadily16,17). These tendency may be due to a change in diet consumption to thin figure and an increase in physical activities, psychological stress affecting menstrual cycles18). The most often demonstrated menstrual disorders are poly-menorrhea, oligomenorrhea, and dys-menorrhea19). These are more frequent among younger adolescents and reach to less frequent 3-5 years after beginning of menarche20).
There have been many studies on the impacts of height, weight, and body structure on the menarche age. However, there is argument for the roles of those components. In this study, we focused on height, weight, body mass index (BMI), menstrual patterns, and menarche age in a large number of late adolescent girls in order to elucidate the influence of menarcheal age on anthropometric indices and menstrual irregularity in late adolescents.
Materials and methods
1. Subjects
This study was performed from June 2008 to October 2009 at seven girl's high schools which approved the survey and including some female college students in Seoul, Korea. The inclusion criterion was adolescent girls who underwent menarche more than 2 years prior to the survey. A total of 4,218 females, aged 16-18 years old, were enrolled in the study and categorized into three groups according to their menarcheal age: early menarche group (younger than 2 standard deviations [SD] of the mean menarcheal age), mid menarche group (between 2 SD of the mean menarcheal age), and late menarche group (older than 2 SD of the mean menarcheal age).
2. Methods
The survey tool was a self-report questionnaire that included questions on anthropometric data (height, weight, and waist circumference), menarcheal age, menstrual irregularity, and frequency of menstruation per year. We calculated BMI using weight and height. The Institutional Review Board of the hospital approved this study, and informed consent was obtained from all parents and participants.
3. Statistical analysis
The data were analyzed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA), and P <0.05 was used to determine statistical significance. The differences among anthropometric indices according to menarche age groups were analyzed by analysis of variance. Multiple comparisons were performed using Tukey test. Correlation analyses were used to investigate associations between menarcheal age and anthropometric indices.
Results
The mean menarcheal age of early menarche group was 9.9±0.2 years, mid menarche group 12.5±0.9 years, and late menarche group 15.1±0.3 years (P = 0.000). The mean height of early menarche group was 160.4±5.2 cm, mid menarche group 161.8±4.9 cm, and late menarche group 162.3±4.7 cm (P = 0.001). BMI was 21.2±2.7 kg/m2 in early menarche group, 20.1±2.4 kg/m2 in mid menarche group, and 19.2±2.4 kg/m2 in late menarche group (P = 0.000). The waist circumference of early menarche group was 70.8±7.5 cm, mid menarche group 68.2±5.7 cm, and late menarche group 67.1±5.9 cm (P = 0.000). There were significant differences between the three menarcheal groups in height, BMI, and waist circumference. BMI and waist circumference were significantly greater among early menarche group compared with mid and late menarche groups. Late menarche group was tallest among the three groups (Table 1).

Anthropometric data in late adolescent girls according to menarcheal groups
The menarcheal age was correlated positively to height (r =0.095, P < 0.001) and was correlated negatively to weight (r =-0.146, P < 0.001), BMI (r =-0.213, P < 0.001), and waist circumference (r =-0.143, P < 0.001) (Fig. 1, Table 2).

Age at menarche and height (A), body mass index (BMI, B), and waist circumference (C) of late adolescent girls.
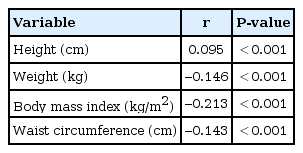
Correlations of age at menarche and anthropometric data
Regular menstruation patterns (more than nine times per year) was 86.7% in early menarche group, 78.9% in mid menarche group, and 63.4% in late menarche group. Oligomenorrhea (less than six times per year) was more common in late menarche group (Fig. 2).

Yearly frequency of menstruation in late adolescent girls according to menarcheal group.
Discussion
Menarche is a vital occurrence in a female life. The downward tendency of menarcheal age has been reported in many countries5,6,21-23), containing Korea. Women born in 1920's had a mean menarcheal age of 17 years, while the mean menarcheal age of women born in 1980's was 14 years7). We also found that the mean menarcheal age was 12.6±1.2 years, confirming the recently decline tendency in Korean aldolescents. However, our participants were limited in the Seoul and not replace the whole Korean female adolescents.
The menarcheal age is influenced by many factors, such as nutrition, emotional stress, geographic and climatic condition, disease and genetic, socio-economic state1-4). The impacts of anthropometric parameters, such as obesity indices and body fat, have previously been reported, but results were controversial7,14,24-27).
Numerous studies have proved a direct association between early menarcheal age and body weight, BMI7,14,24-27). Although the mechanisms including to the inverse association between obesity and menarcheal age are not completely discovered, it has been reported that the speed of sexual maturation and body fat mass can affect this relationship14). Frisch and Revelle24) found that the part of body fat acts as a endo-neurocrine stimulants in menarche event. In contrast, Garcia Cuartero et al.28) found no correlation between menarcheal age and BMI, and Demerath et al.29) showed that the menarcheal age was not reliant on BMI.
Girls who experience menarche early are likely to be more heavier in adulthood life14,30,31). These studies showed that late adolescent girls who underwent an early menarche had a lager BMI and waist circumference than mid and late menarche groups. We demonstrated an inverse association between menarcheal age and BMI and waist circumference in late adolescent girls. These results suggest that early sexual maturation triggers body fat mass accumulation. The upward tendency of adult obesity prevalence among early menarche group may largely represent the continuation of child obesity until adulthood later31). The inverse association of menarcheal age with BMI and obesity in middle aged women is not explained entirely by early childhood BMI. Instead, menarcheal age is probably a surrogation indicator for the speed of sexual maturation, which leads to different fat accumulation in the peripubertal period, and this continues into adulthood life30). Although the fine endo-biological processes of the inverse association between menarcheal age and adulthood obesity prevalence are uncertain, it has been suggested that girls who undergo menarche early may have a longer period of a positive energy balance or that many endo-neurocrine stimulants influence the speed of sexual maturation and the obesity14).
Global increasing tendency have been demonstrated for adult height as well as downward tendency for menarcheal age since the 1900's. The taller height tendency is likely caused by alterations to nutrition, health status15). Several studies have shown that women who undergo menarche earlier have a shorter final adult height compared with women who experience menarche later15,32). A study of 286,205 European women found that latest birth group has a earlier menarcheal age and a taller height, presenting that women who undergo menarche later will finally grow taller than women who undergo menarche earlier15). This positive association between menarcheal age and final adult height may be accounted by the earlier shutdown of plates due to the female estrogen hormone increment. Therefore, the menarcheal age perhaps has major roles on long bone growth15,32). The height of menstruated girls is considerably taller than nonmenstruated girls33), but an earlier shutdown of the plates may lead to a shorter final height at adulthood15,32). In our study, the menarcheal age was correlated positively to height in late adolescent girls who had reached to their final adult height; the mean age of these subjects was 17.3 years and their height was likely to that of the final adult height.
Immediately after beginning of menarche, there is a temporary period with anovulatory cycles previous to ovulatory cycles. Few data are valid on the beginning age of regular menstrual cycle. Several studies have shown an upward tendency of anovulatory cycles with increasing menarcheal age16,17,34-36). Apter35) found that these tendency was influenced by the menarcheal age, that is, earlier menarche girls who experienced menarche before 12 years have a more rapid onset of ovulatory menstrual cycles than girls having later menarche. Similarly, Hosokawa et al.17) found that Japanese women who underwent menarche later were delayed regular menstrual cycle. The proportion of women who experienced the onset of regular menstrual cycles at 5 years and more after menarche was 26%, 30%, 37% for early (age at menarche <10 years), mid (age at menarche 11-14 years), late (age at menarche>15 years) menarche group, respectively (P <0.0001). In a United States study, the interval period from menarche to the foundation of regular menstrual cycle was reported slightly positive association with menarcheal age36). Our results also showed that oligomenorrhea was more common in late menarche group.
There are many hypotheses for oligomenorrhea in adolescence. A premature hypothalamus-pituitary-ovary axis may tend to oligomenorrhea and an anovulatory menstrual cycle17,19). Anovulatory cycles are often found in the moment immediately after beginning of menarche, with menstrual cycles being irregular before enhancing of a positive feedback in the central nervous system result in the starting of regular menstrual cycle17). Irregular menstrual cycles have a crucial role on various female health conditions including psycho-social problem, infertility, and cardiovascular disorders in advanced age37). In French women study, the age at beginning of regular menstrual cycle increased gradually and presented a profound increase in the period between menarcheal age and at beginning of regular menstrual cycle16). Further studies are needed to identify the endo-neurocrine components connected to early menarche and the age at beginning of regular menstrual cycles.
Our study had some limitations. First, we used a cross sectional study design so that causality could not be determined. Second, the menarcheal age and anthropometric indices were gathered through self-reported questionnaires. Anthropometric indices were not directly measured through objective devices. The accuracy of recall of the data reliance on many factors, including of the interval term of recall, which has been reported to be a credible and logical tools for estimating age at menarche38). In our study, the mean interval term of recall was 4.6 years (time of interview age, 17.2±0.7 years; mean menarche age, 12.6±1.2 years). Consequently, we assumed that recall bias would be low due to the short interval term of recall. Third, we did not collect data that are known to be associated with menarcheal age, including physical activity, diet consumption, socio-economic and nutritional status.
A strong point of this study was our large participants number (n=4,218) of late adolescent girls; this is the largest study investigating the influence of menarcheal age on anthropometric indices and menstrual irregularity in Korea.
In conclusion, we found a significant inverse relationship between menarcheal age and obesity and a positive relationship between menarcheal age and height. Girls who experience menarche later had a higher risk for menstrual irregularity in late adolescent girls in Korea. Further long term cohort investigations are needed to fully explain these causal relationships.
Acknowledgments
The work was supported by the Ewha Global Top 5 Grant 2013 of Ewha Womans University.
Notes
No potential conflict of interest relevant to this article was reported.