Introduction
Metabolic syndrome (MetS) is known as a major risk factor in cardiovascular disease, diabetes, and cerebral vascular disease1,2,3,4,5,6,7,8,9), and it has become a very important public problem due to the worldwide increased prevalence of obesity in adults10). According to South Korean reports, the local prevalence rate of obesity in children and adolescents is increasing rapidly11), and is closely related to MetS-related disorders, such as cardiovascular disease, diabetes, and hyperlipidemia12). As MetS at young age is so closely connected to that in adulthood, early selection of at-risk groups and early management are very important13). The widely reported variation in the prevalence rate of MetS in childhood is due to the absence of a unifying definition of this condition in childhood14).
Considering that insulin resistance (IR) is a cause of MetS, it is possible to screen at-risk groups for childhood MetS15). Although direct measurements of IR are possible with the pancreatic suppression test and hyperinsulinemic euglycemic glucose clamp technique, these direct tests are invasive, complex, and expensive16). Therefore, clinical use of these methods is limited during childhood. Instead, indirect index, such as the homeostasis model assessment of IR (HOMA-IR), is widely used clinically17). Based on the findings that elevation of serum triglyceride (TG) is related to a decrease in insulin sensitivity18) by interfering with muscle glucose metabolism19), another indirect index, the TG and glucose index (TyG index), has been used in some adult studies20,21,22). The TyG index is based on fasting TG and glucose instead of fasting insulin and glucose. Given the high cost incurred in insulin measurement and the absence of a standard measurement method, the clinical application of the TyG index is convenient. However, there are few pediatric studies and reference criteria in Korea.
The aim of the present study was to calculate the prevalence of MetS, tabulate the distribution of the percentile values of the HOMA-IR and TyG index, and propose a cutoff value to classify an at-risk MetS group among Korean children and adolescents.
Materials and methods
1. Subjects
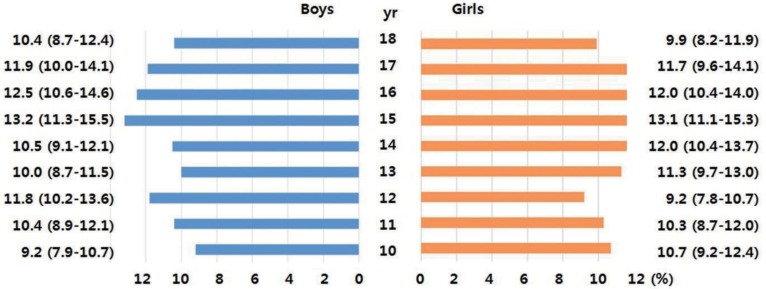
Primary data were obtained from the fourth and part of the fifth Korean National Health and Nutrition Examination Survey (KNHANES, 2007ŌĆō2010). These surveys are conducted periodically by the Division of Health and Nutrition Survey, Korea Center for Disease Control and Prevention of the Ministry of the Health and Welfare. The KNHANES consists of health- and nutrition-related questions and health examinations of a sample of people selected from across the country every year. Among the 4,244 children and adolescents aged 10ŌĆō18 years who participated in the survey, 3,313 (1,756 boys and 1,557 girls) individuals were included in the final analysis after excluding 931 individuals with missing data on body measurements or inadequate blood test results (i.e., without fasting for 8 hours). The age distribution of the participants by weighted sampling is shown in Fig. 1.
2. Health screening and measurement of biochemical indies
A team who took part in regular education training and evaluation each year collected all the data. The waist circumference (WC) was measured at the mid-point between the lower end of the rib and upper end of the ilium. After the subjects had rested for 5 minutes in a sitting position, their blood pressure (BP) was measured by the duty nurses using Baumanometer desk model 0320 (Baum Co., Copiague, NY, USA). Three measurements of the systolic and diastolic BP were recorded, and the average value was used in the analyses.
Venous blood samples were collected after fasting 8 hours, and were analyzed at the central laboratory (Seoul Medical Science Institute, Seoul, Korea in 2007; MEODIN Medical Institute, Seoul, Korea in 2008ŌĆō2010). Fasting glucose, TG, and high-density lipoprotein cholesterol were analyzed by an enzyme assay (Hitachi Automatic Analyzer 7600, Hidachi, Tokyo, Japan), and fasting insulin was analyzed using a gamma counter (1470Wizard, Perkin-Elmer, Turtu, Finland) with an immunoradiometric assay (INS-IRMA, Biosourse, Belgium). Health screening and measurement of biochemical indices were described according to the guidebook of the fourth and fifth KNHANES23,24).
3. Definitions
This study used 3 of the most commonly used criteria for MetS in children and adolescents (Table 1): those of Cook et al.25) and de Ferranti et al.26), ŌĆō modified from the National Cholesterol Education Program Adults Treatment Panel III, and those of the International Diabetes Federation (IDF)27), The HOMA-IR and TyG index were used as indirect indies of IR. HOMA-IR was calculated as follows: HOMA-IR=fasting insulin (┬ĄU/mL)├Śfasting glucose (mmol/L)/22.5. The TyG index was calculated as follows: TyG index=Ln [triglyceride (mg/dL)├Śfasting glucose (mg/dL)/2]17,20).
4. Statistics
Statistical analysis was performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Variables are presented as means with their 95% confidence intervals (CIs). The following percentile values of the HOMA-IR and TyG index were calculated: 10th, 25th, 50th, 75th, and 90th. Receiver operation characteristic (ROC) analysis and the area under the curve (AUC) were used to identify the sensitivity and specificity for HOMA-IR and TyG index, respectively. The optimal cutoff values were defined as the point at which the value of "sensitivity + specificity -1" was maximum (Youden index). This cutoff value corresponds to the point on the ROC curve which has the maximum vertical distance from the curve to the chance line.
Results
The general characteristics of the participants are shown in Table 2. The highest prevalence rates of MetS in males and females were 13.9% and 12.3%, respectively, according to the criteria of de Ferranti et al., and the lowest prevalence rates were 1.4% and 1.8%, respectively, according to the IDF criteria. The prevalence rates of MetS for males and females using the criteria of Cook et al. were 4.6% and 3.6%, respectively, so fell somewhere in the middle of the rates estimated by the other criteria. The clinical characteristics of the participants with MetS are shown in Table 3.
The mean values of HOMA-IR were 2.97 (95% CI, 2.90ŌĆō3.04) in males and females, 2.92 (95% CI, 2.83ŌĆō3.00) in males, and 3.03 (95% CI, 2.93ŌĆō3.13) in females. The mean values of the TyG index were 8.13 (95% CI, 8.11ŌĆō8.16) in total males and females, 8.11 (95% CI, 8.08ŌĆō8.14) in males, and 8.15 (95% CI, 8.13ŌĆō8.19) in females. The percentile distributions of the HOMA-IR and TyG index are shown in Table 4.
The ROC curves of the HOMA-IR and TyG index for MetS according to the three criteria are displayed in Fig. 2. AUC of the HOMA-IR and TyG index was 0.783 and 0.915, respectively, using the criteria of Cook et al.; 0.742 and 0.878, respectively, using the criteria of de Ferranti et al.; and 0.827 and 0.940, respectively, using the criteria of the IDF. The cutoff values of the HOMA-IR and TyG index according to the ROC curves are tabulated in Table 5. The cutoff values of the HOMA-IR and TyG index were 3.29 and 8.48, respectively, according to the criteria of Cook et al.; 2.96 and 8.41, respectively, according to the criteria of de Ferranti et al.; and 3.54 and 8.66, respectively, according to the criteria of the IDF. The sensitivities and specificities of the cutoff values for the HOMA-IR and TyG index are tabulated in Table 5.
Discussion
During childhood and adolescence, the physical and physiological changes according to the age and sex are so enormous, that a unified standard for MetS cannot be estimated. As a result, the exact prevalence of MetS in Korean children and adolescents is not known. We used three well-known criteria and data from the fourth and fifth KNHANES to calculate the prevalence of MetS. The prevalence of MetS in children and adolescents varied, from 1.4% to 13.9%. The prevalence rates in males and females were lowest (1.4% and 1.8%, respectively) using the criteria of the IDF and highest using the criteria of de Ferranti et al. (13.9% and 12.3%, respectively). The inclusion of central obesity and a higher TG level were responsible for the low prevalence rates using the IDF criteria. The high rate using the criteria of de Ferranti et al. was due to the use of a lower TG level. The prevalence of MetS in Europe and the United States was 2.6% and 2.2%, respectively, using the IDF criteria28), higher than the prevalence found in the present study. The discord in the results may be due to the higher obesity rate in Europe and the United States.
In this study, we tried to confirm the percentile distribution of indirect indices of MetS, such as HOMA-IR and TyG in Korean children and adolescents, and to analyze the ability of these indirect indices to diagnose MetS with the aim of, suggesting cutoff values to screen at-risk groups of MetS.
In the ROC curve analysis of the correlation between the indirect indices and MetS, the AUC of the TyG index was larger than that of the HOMA-IR using all three criteria (Fig. 2). The TyG index uses 2 measures of fasting glucose and TG, whereas HOMA-IR uses only one measure of fasting glucose in MetS (Table 1). Based on the results of this study, the TyG index seemed to be a more useful screen than HOMA-IR to determine the risk of MetS. Both the TyG index and HOMA-IR were reported to reflect the IR in healthy adult29), and TyG index was better associated with carotid atherosclerosis than HOMA-IR in a report30). In hyperglycemic clamp validated study, correlation for the TyG index was better compared with HOMA-IR in adult population22). However, from a practical point of view, the TyG index is not useful to ascertain IR in children because it has not been widely applied in the pediatric field. Thus, it is difficult to compare the superiority of the index with that of HOMA-IR. We suggest that the TyG index could be used as an ancillary measure to support the HOMA-IR method.
For screening, the cutoff point used in this study was the highest value of the Youden index in the area of highest sensitivity rather than specificity. The cutoff values of the HOMA-IR and TyG index using the criteria of Cook et al. were 3.29 and 8.48, respectively, which are close to the 75th percentile in healthy children and adolescent distribution. The cutoff values using the criteria of de Ferranti et al. were located between the 50th and 75th percentiles, and the values determined by the IDF criteria were between the 75th and 90th percentiles. We attributed these discrepancies to the different MetS definitions of the three criteria. The criteria of the IDF are stricter than those of Cook et al., whereas those of de Ferranti et al. are less strict than Cook et al.'s criteria (Table 1). The stratification of an at-risk group using the three criteria may be helpful, however, the clinical usefulness of the criteria needs to be verified in further studies.
The present study has some limitations. One of the limitations was not discriminating children and adolescents. During the pubertal period, IR increases at the onset of puberty, but it returns to prepubertal levels by the end of puberty31). In cases of obesity, the increases in the level of IR during puberty are more pronounced, and these do not return to prepubertal levels at the end of puberty32). Although the subgroups in the present study were analyzed according to the age or puberty, the ROC curves were not meaningful because of the low incidence of MetS. Additional studies of the influence of puberty on IR are needed. The other limitation was that the HOMA-IR and TyG index represent indirect rather direct indices of IR.
In conclusion, we suggested three different cutoff points to screen at-risk groups of Korean children and adolescent for MetS using HOMA-IR and TyG index.