Sitosterolemia: a review and update of pathophysiology, clinical spectrum, diagnosis, and management
Article information
Abstract
Sitosterolemia is an autosomal recessive disorder characterized by increased plant sterol levels, xanthomas, and accelerated atherosclerosis. Although it was originally reported in patients with normolipemic xanthomas, severe hypercholesterolemia have been reported in patients with sitosterolemia, especially in children. Sitosterolemia is caused by increased intestinal absorption and decreased biliary excretion of sterols resulting from biallelic mutations in either ABCG5 or ABCG8, which encode the sterol efflux transporter ABCG5 and ABCG8. Patients with sitosterolemia show extreme phenotypic heterogeneity, ranging from almost asymptomatic individuals to those with severe hypercholesterolemia leading to accelerated atherosclerosis and premature cardiac death. Hematologic manifestations include hemolytic anemia with stomatocytosis, macrothrombocytopenia, splenomegaly, and abnormal bleeding. The mainstay of therapy includes dietary restriction of both cholesterol and plant sterols and the sterol absorption inhibitor, ezetimibe. Foods rich in plant sterols include vegetable oils, wheat germs, nuts, seeds, avocado, shortening, margarine and chocolate. Hypercholesterolemia in patients with sitosterolemia is dramatically responsive to low cholesterol diet and bile acid sequestrants. Plant sterol assay should be performed in patients with normocholesterolemic xanthomas, hypercholesterolemia with unexpectedly good response to dietary modifications or to cholesterol absorption inhibitors, or hypercholesterolemia with poor response to statins, or those with unexplained hemolytic anemia and macrothrombocytopenia. Because prognosis can be improved by proper management, it is important to find these patients out and diagnose correctly. This review article aimed to summarize recent publications on sitosterolemia, and to suggest clinical indications for plant sterol assay.
Introduction
Sitosterolemia, also known as phytosterolemia, is an autosomal recessive disorder characterized by increased plant sterol levels, xanthomas, and accelerated atherosclerosis12). It is caused by increased intestinal absorption and decreased biliary excretion of plant sterols resulting from homozygous or compound heterozygous mutations in either ABCG5 or ABCG8, which encode the sterol efflux transporter ABCG5 (sterolin-1) and ABCG8 (sterolin-2) that pumps sterols out to intestinal lumen or into bile34). Although it is a rare disease, it is an important disease that led to understanding of the physiologic pathway about sterol influx and efflux56).
Mediterranean stomatocytosis/macrothrombocytopenia has been identified as the hematological presentation of sitosterolemia7). Stomatocytic hemolysis, large platelets, splenomegaly, and abnormal bleeding can be associated, and hematologic manifestations can be the only clinical sign of sitosterolemia8). The true prevalence of sitosterolemia is unknown due to underdiagnosis, and sitosterolemia may be more frequent than previously thought. One Asian individual with sitosterolemia was identified incidentally out of 2,542 persons from a study in which plasma plant sterols were analyzed9).
Because delayed diagnosis can lead to poor clinical outcome due to advanced atherosclerotic cardiovascular disease and prognosis can be improved by proper management including plant sterol restriction and cholesterol absorption inhibitor in sitosterolemia, it is important to find these patients out and diagnose correctly2810). This review article aimed to summarize recent publications on the pathophysiology, clinical spectrum, diagnosis and management of sitosterolemia, and to suggest clinical indications for plant sterol assay.
The plant sterols
Plant sterols are rich in vegetable oils, wheat germs, nuts, seeds, avocados, chocolate, and margarine26). They are structurally very similar to cholesterol, but they differ by the presence of an ethyl or methyl group (sitosterol and campesterol, respectively) or a double bond (stigmasterol)1). Sitosterol is usually the most abundant plant sterol in the diet and the predominant form found in patients with sitosterolemia811).
Average Western diet contains similar amount of cholesterol and plant sterols. Although approximately 50% of dietary cholesterol is absorbed, less than 5% of plant sterols are absorbed in normal individuals611). High plant sterol diet was extremely toxic in animal models of sitosterolemia, and it was suggested that the mammalian body defends itself against plant sterols because they are toxic when accumulated, although similar toxicity have not been documented in human yet1213).
It is clear that plant sterols are toxic to those with sitosterolemia, but plant sterol intake seems to be safe to nonsitosterolemic individuals. Instead, plant sterols can competitively inhibit cholesterol absorption, and the cholesterol lowering effect of plant sterols have been documented11). Although they have not been shown to reduce clinical outcomes, many cholesterol lowering functional foods are enriched with plant sterols1415). On the other hand, studies have raised the possibility of association between plant sterol levels and atherosclerosis1617). The cholesterol lowering effect may compensate the potential risk of increased plant sterol intake911), and the debate whether plant sterol is beneficial or harmful is still ongoing1518).
Sterol absorption in normal subjects
Dietary cholesterol and noncholesterol sterols, mainly plant sterols and stanols (saturated sterols), are absorbed form the intestinal lumen via the sterol influx transporter, Nieman Pick C1 Like 1 (NPC1L1)6). The NPC1L1, the gatekeeper of sterol absorption, have lower affinity to plant sterols than cholesterol1920). After absorption to the enterocytes, about 50%–60% of cholesterol is esterified by the acetyl-sterol O-acyltransferase 2 (SOAT2) and transported to liver packed in the chylomicrons21). Unesterified cholesterol or plant sterols are pumped back to intestinal lumen by ABCG5/ABCG8, the sterol efflux transporters6). The SOAT2 also have low affinity with plant sterols, allowing preferential plant sterol efflux by the ABCG5/ABCG822). Plant sterols not pumped back to the intestinal lumen become part of the chylomicrons, transported to the liver, and eventually pumped out into the bile by the hepatic ABCG5/ABCG8 transporters611).
Disrupted sterol homeostasis in sitosterolemia
Biallelic defects in either ABCG5 or ABCG8 result in increased intestinal absorption and decreased biliary excretion of plant sterols, leading to extremely high plasma levels of plant sterols34). Patients with sitosterolemia absorb 15% to 60% of ingested sitosterol, which lead to a 50- to 200-fold increase in their plasma sitosterol levels13). Plant sterols comprise 15% to 20% of total plasma sterols in patients with sitosterolemia and are carried in low-density lipoprotein (LDL) and very-LDL particles323).
In a patient with liver failure and sitosterolemia that underwent liver transplantation, the elevated plant sterol levels decreased to values less than 1/10 of pretransplantation level, suggesting that the liver functions as the predominant organ for maintaining sterol balance24). ABCG5/ABCG8 expression either in liver or intestine protected animals from sterol accumulation in a recent study25).
Although sterol absorption was moderately increased in heterozygotes, they are asymptomatic with normal cholesterol levels and normal to slightly increased plant sterol levels126).
Clinical spectrum of sitosterolemia
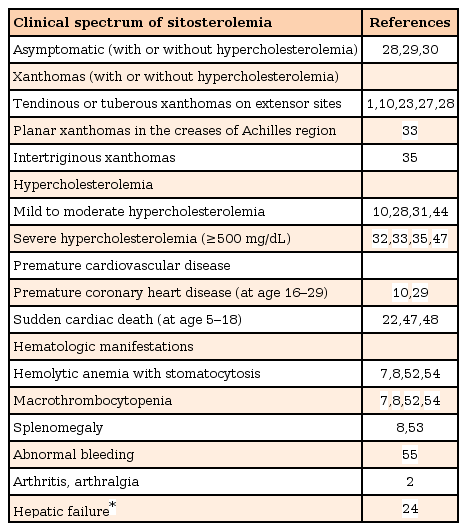
Patients with sitosterolemia show extreme phenotypic heterogeneity. Whereas some patients with homozygous mutations are almost totally asymptomatic, others show severe hypercholesterolemia leading to accelerated atherosclerosis and premature cardiac death127282930). A 10-year-old girl from Iran, who had received almost vegetable-free diet in Iran and started to intake much more vegetables and olive oil after her family moved to Europe, developed xanthomas and hypercholesterolemia in a short period of time and was finally diagnosed for sitosterolemia31). Although the amount of dietary plant sterol intake should be at least partially related with the severity of clinical disease, the mechanism of phenotypic heterogeneity, even between the family members that shares same gene and environment, is not fully understood yet. A recent report in a Chinese family with sitosterolemia suggested potential effects of NPC1L1 polymorphisms in protecting against clinical disease29). Major clinical features of sitosterolemia, especially in young patients with sitosterolemia are summarized in Table 1.
Clinical spectrum of sitosterolemia
1. Hypercholesterolemia
Although it was originally reported in patients with normolipemic xanthomas27), cholesterol absorption is also increased in patients with sitosterolemia, and serum cholesterol levels are usually elevated110). Very high levels of cholesterol (up to 1,000 mg/dL) have been reported in patients with sitosterolemia, especially in children3233). Immature intestine may absorb higher amounts of cholesterol compared with that of adults34).
Breastfed infants with sitosterolemia show unique clinical features323335). The plant sterol intake of a breastfed infant should be minimal because the plasma sitosterol levels of the heterozygote mother should be only slightly increased. However their cholesterol intake can be high due to high cholesterol content of human milk (90–150 mg/L vs. 0–4 mg/L in human milk and infant formula, respectively)36). Breastfed infants with sitosterolemia can present with extremely high cholesterol levels with xanthomatosis, but with normal sitosterol:cholesterol ratio due to only mildly elevated plant sterol levels33). The plant sterol level increase and the cholesterol level somewhat decrease as the infant start taking fruits and vegetables3335).
2. Xanthomas
Tendinous or tuberous xanthomas on extensor areas, such as Achilles tendon, extensor tendons of the hand, elbows and knees are the major clinical manifestations of sitosterolemia12327). Minor trauma plays an important role in the development of xanthomas, and this is why they appear on extensor surfaces in most patients37).
Xanthomatosis is rarely observed in young children, and when present, homozygous familial hypercholesterolemia (FH) or autosomal recessive hypercholesterolemia is most often suspected3738). Xanthomas may begin to appear at very young age in sitosterolemia, sometimes during the first year of life3335).
Intertriginous xanthomas are a very rare type of planar xanthomas and have been reported to be pathognomonic for homozygous FH39). However, intertriginous xanthomas (first noticed at the age of 3 months when the patient was being exclusively breastfed) were observed in a 15-month-old Korean girl with sitosterolemia, suggesting that intertriginous xanthomas may develop in young children with extremely high cholesterol levels of any etiology35). Friction between the skins in intertriginous areas may contribute to the development of xanthomas in a chubby infant in whom extensor areas are relatively spared because movement is not active yet.
Most sitosterolemic patients with severe atherosclerotic cardiovascular disease also showed xanthomas1102328). Xanthomas evolve as clusters of foam cells in the skin, and the mechanisms involved in the development of xanthoma seem to be similar to those in early stages of atherosclerotic plaques40). According to a meta-analysis on patients with genetic diagnosis of FH, the presence of tendon xanthomas was associated with a 3.2 times higher risk of cardiovascular disease41). Xanthelasma of the eyelids was considered to be only a cosmetic lesion until recently, however recent prospective studies showed that it is connected with an increased cardiovascular risk and reduced average lifespan42). In contrast to the initial case with normolipemic xanthomas27), xanthomas regress and sometimes completely disappear in some patients with sitosterolemia, usually associated with dramatically decreased plasma cholesterol levels, although plant sterol levels were still relatively high323543444546).
3. Atherosclerotic cardiovascular disease
Some patients with sitosterolemia develop premature atherosclerosis leading to sudden cardiac death at as early as 547),1348),1822) years of age, whereas others, even in the same family of symptomatic patients, do not show any classic sign of sitosterolemia242835).
Both elevated plasma cholesterol and plant sterol levels can contribute to the premature vascular disease in patients with sitosterolemia. Accumulation of plant sterol in plasma lipoproteins influences the stability of both cholesterol and plant sterol in lipoproteins, favoring the accumulation of these sterols within tissues, initiating inflammatory reactions, and may cause premature atherosclerosis6).
Coronary plaque disruption and superimposed thrombosis is the major cause of acute myocardial infarction and sudden cardiac death49). The composition and vulnerability of plaque rather than its volume or the severity of stenosis are more important for the development of the thrombus-mediated acute coronary syndromes49). Plant sterols are relatively poorly esterified by the sterol-esterifying enzyme acyl-CoA-cholesterol acyl transferase. Macrophages incubated with sitosterol-containing lipoproteins accumulated free sterols and underwent necrotic cell death, which may contribute to the formation of rupture-prone plaque50).
Premature coronary heart disease can develop in sitosterolemic patients with normal cholesterol levels. A 16-year-old sitosterolemic girl with normal cholesterol level was reported to have premature coronary heart disease requiring coronary bypass grafts51), and a normocholesterolemic patient who underwent a 3 vessel coronary bypass surgery at the age of 29 was diagnosed with sitosterolemia after that10).
On the other hand, Hansel et al.30) could not find significant signs of premature atherosclerosis in 5 patients with sitosterolemia aged 11 to 21 years, in spite of severe hypercholesterolemia as well as extremely high plant sterol levels. They suggested that the premature atherosclerosis in some patients with sitosterolemia may be due at least in part to mechanisms independent of elevated circulating plant sterol levels30).
4. Hematologic manifestations
Rees et al.7) revealed that stomatocytic hemolysis and macrothrombocytopenia (previously known as the Mediterranean stomatocytosis or Mediterranean macrothrombocytopenia, which had been a poorly understood hematological condition) is the hematological presentation of sitosterolemia.
Stomatocysis, hemolytic anemia, thrombocytopenia with very large platelets, splenomegaly, and abnormal bleeding can be associated with sitosterolemia8). Because the ABCG5 and ABCG8 are only expressed in intestine and liver, acquired accumulation of circulating plant sterols and their incorporation into red blood cells (RBC) and platelet seems to be resulting in abnormal morphology and function7).
Blood cells can be a main target for the toxic effect of plasma plant sterols, and sitosterolemia can be manifested mainly by hematologic abnormalities52). Three patients from a Chinese family, all of whom had suffered from severe hemolytic anemia and macrothrombocytopenia since 3 to 4 years of age and underwent splenectomy in their 10's, was diagnosed as sitosterolemia in their 20's. All of these patients had increased plasma sitosterol but normal cholesterol levels52). Thirteen sitosterolemic patients with hematologic manifestations, including 2 patients without any classical features of sitosterolemia, had been misdiagnosed with immune thrombocytopenia (ITP), Evans syndrome, or secondary ITP with delay being 15 to 49 years between symptom onset and correct diagnosis53). Plasma plant sterols should be analyzed in patients with unexplained hemolytic anemia with macrothrombocytopenia to avoid unnecessary splenectomy54).
Recently, Kanaji et al.55) have identified that the bleeding abnormalities and macrothrombocytopenia associated with sitosterolemia are due to direct plant sterol incorporation into the platelet membrane, resulting in platelet hyperactivation, reduced αIIbβ3 surface expression, loss of the GPIba-FlnA linkage, microparticle formation, and ultimately poor hemostatic functions.
Diagnosis of sitosterolemia
Routine laboratory methods do not distinguish plant sterols from cholesterol, and a more accurate method such as gas chromatography-mass spectrometry (GC-MS) is required. Measurement of serum plant sterol by GC-MS or liquid chromatography-mass spectrometry is regarded as a reliable test for screening sitosterolemia, in which unequivocally increased plant sterol levels and sitosterol: cholesterol levels are almost invariably observed1).
Genetic confirmation can be given by direct sequencing of exons and intron-exon boundaries of the ABCG5 and ABCG8 genes, each comprised of 13 exons and located in a head-to-head organization on chromosome 2p21, and documenting the homozygous or compound heterozygous mutations in either ABCG5 or ABCG834). Asian patients usually have mutations in ABCG5, while Caucasian patients usually have ABCG8 mutations332). However, mutations in ABCG8 have been reported in 3 of 8 families with hematologic manifestations of sitosterolemia according to a recent Chinese study, suggesting that ABCG8 mutations are not exclusive to Caucasians53). DNA sequencing of ABCG5/ABCG8 is should be performed to rule out sitosterolemia in breastfed infants, because they can exhibit only mild elevation of plasma sitosterol level and normal sitosterol:cholesterol ratio33).
In contrast to patients with homozygous FH that are relatively refractory to dietary modification and cholesterol-lowering agents, plasma cholesterol levels in sitosterolemic patients are extremely sensitive to dietary cholesterol restriction and bile acid sequestrants324344).
The entire pathway of cholesterol biosynthesis including hepatic hydroxymethylglutaryl coenzyme A (HMG CoA) reductase is exceptionally down-regulated in patients with sitosterolemia1056). It was also reported that stigmasterol and campesterol inhibit activation of sterol regulatory binding protein-2 (SREBP-2), a transcription factor involved in cholesterol biosynthesis, in cultured adrenocortical cells57), and that stigmasterol, not sitosterol, inhibits processing of SREBP-2 leading to reduced cholesterol synthesis in mice58).
In nonsitosterolemic individuals, cholesterol synthesis increases after sterol depletion, limiting the effect of sterol absorption inhibitor or bile acid sequestrant57). However, there is no such compensatory increase in cholesterol synthesis in those with sitosterolemia, resulting in dramatic reduction in plasma cholesterol levels59). Sitosterolemia should be suspected when the plasma cholesterol falls more than 40% on a low-cholesterol diet.
Sitosterolemia seems to be significantly underdiagnosed, and many of these patients should be continuing to intake large amount of plant sterols, not knowing that the plant sterols are 'toxic' to them, but believing that those food are good for their health. Sitosterolemia might also be significantly underdiagnosed in children in whom screening for lipid profiles is not universally performed. Recent guidelines recommend screening all children at 9–11 years and again at 17–21 years to find those with hypercholesterolemia60). Some of those screened may in fact have sitosterolemia, and these patients may be distinguished by either remarkable response to dietary modification or poor response to statins35).
Management of sitosterolemia
Management of sitosterolemia aims to reduce plasma plant sterol (as low as possible; although perfect control [sitosterol level <1 mg/dL] cannot be achieved) and cholesterol concentrations and to prevent or reduce xanthomas and atherosclerotic cardiovascular diseases2).
Mainstay of therapy is dietary restriction of both cholesterol and plant sterols. Foods rich in plant sterols include vegetable oils, wheat germs, nuts, seeds, avocado, most of which are known to be heart-healthy foods261). Margarine, shortening, and chocolate should also be avoided. Polished rice should be taken instead of whole grains. Shellfish and seaweeds contain significant amount of algae-derived plant sterols that are also hyperabsorbed in these patients, and they should also be avoided62). However, plant sterol-free diet is almost impossible to accomplish because plant sterols are found in almost every plant-based foods, and low plant sterol diet have resulted in only about 30% reduction of plasma plant sterol levels1144).
Pharmacotherapy include the sterol absorption inhibitor, ezetimibe, or bile acid sequestrants such as cholestyramine. Patients with sitosterolemia usually do not respond to statins because HMG CoA reductase activity is already maximally inhibited60).
The bile acid sequestrants inhibit the reabsorption of bile acids in the ileum and disrupt the enterohepatic circulation of bile acids. The bile acid sequestrants was reported to reduce plasma plant sterol levels by up to 45%, although they may result in more dramatic decrease in plasma cholesterol levels (50%–80%) and regression of xanthomas4344). Sitosterolemia should be considered in patients with hypercholesterolemia and/or xanthomas who show dramatic reduction of cholesterol levels or regression of xanthomas by bile acid sequestrant therapy. However, poor compliance and gastrointestinal side effects limit the use of cholestyramine.
Ezetimibe, an inhibitor of intestinal sterol absorption through its binding to NPC1L1, is currently considered the choice of treatment for sitosterolemia63). It has been widely used for decreasing serum LDL-cholesterol levels in patients with hypercholesterolemia. Ezetimibe also reduces the intestinal absorption of plant sterols, thereby also lowering plasma plant sterol levels. Ezetimibe alone or in combination with cholestyramine successfully decreased plasma cholesterol and plant sterol levels (about by 50%; although still much higher than normal values)63), resulting in regression of xanthomas and improvement of carotid bruits and cardiac murmurs in patients with sitosterolemia45). Long-term treatment with ezetimibe 10 mg/day was safe, tolerable, and effective in reducing plasma plant sterol concentrations in patients with sitosterolemia6164). Ezetimibe reduced plasma and RBC plant sterol levels, while increasing platelet count and decreasing mean platelet volume, and thereby may reduce the risk for bleeding in sitosterolemia65).
Although pharmacotherapy is usually not performed for children under age 10, an individual with extremely high levels of cholesterol may begin therapy earlier66) Ezetimibe therapy seems to be also safe and effective in children with sitosterolemia, although an infant did not respond to ezetimibe therapy at 7 months of age possibly due to immature glucuronidation system, who finally showed improvement when ezetimibe was restarted at 2 years of age32). Bile acid sequestrants such as cholestyramine can be added for those with insufficient response to ezetimibe263).
Arthritis and arthralgia can also be associated with sitosterolemia, and more strict management of sitosterolemia can be helpful2).
Conclusions
Plant sterol assay should be performed in patients with normocholesterolemic xanthomas, hypercholesterolemia with unexpectedly good response to dietary modifications or to cholesterol absorption inhibitors, or hypercholesterolemia with poor response to statins, or those with unexplained hemolytic anemia and macrothrombocytopenia (Table 2).

Indications for plant sterol assay
The dramatic cholesterol reduction and regression of xanthomas by proper treatment including plant sterol restriction and cholesterol absorption inhibitor suggest that sitosterolemia can be a controllable condition, and it is important to find these patients out and diagnose correctly because prognosis can be improved by early diagnosis and proper management.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.