Highlights
We conducted a study of haemostatic status of children with T1DM, its change over time and its relationship with the degree of glycaemic control. We found high levels of fibrinogen, plasminogen activator inhibitor-1, von Willebrand factor antigen, a prothrombotic state and micro- and macrovascular complications risk.
Introduction
Type 1 diabetes mellitus (T1DM) is one of the most common endocrine and metabolic diseases in childhood, and its incidence is increasing rapidly. In 2020, the diabetes burden is expected to double, mainly in young people and in adults with a moderate genetic susceptibility [1].
Hyperglycemia can produce molecular changes that alter hemostasis and induce a proinflammatory, prothrombotic, and antifibrinolytic microenvironment [2]. The main components of the hemostatic system affected by hyperglycemia are fibrinogen (Fg), plasminogen activator inhibitor-1 (PAI-1), von Willebrand factor antigen (vWF:Ag), and antithrombin. The increase in Fg level has been associated with coronary artery disease in patients with T1DM. Hyperfibrinogenemia causes increase in coagulation activity, clot strength, and blood viscosity and is a marker of inflammatory vascular modifications and endothelial dysfunction. Moreover, Fg contributes to development and activation of atheromatous plaque [3].
PAI-1 is present in platelets and is produced by endothelial tissue and adipocytes. It is the main endogenous inhibitor of the fibrinolytic system. A clear association has been observed between te increase in PAI-1 plasma level and prothrombotic diseases such as hypertension, obesity, insulin resistance, and diabetes [4,5].
vWF:Ag is a glycoprotein selectively produced by endothelial cells and megakaryocytes. It plays an essential role in hemostasis because it prevents proteolytic degradation of Factor VIII and promotes platelet adhesion and aggregation to damaged endothelium. In addition, Factor VIII mediates vascular inflammation by causing leukocyte recruitment and extravasation and activating the complement cascade. Recently, it has been proposed as a prognostic marker of metabolic and cardiovascular diseases, such as diabetes, myocardial infarction, or stroke [6,7].
In diabetic patients, thrombus is more resistant to degradation in the presence of an increase in PAI-1 level [8,9]. Although macrovascular complications of T1DM in childhood are rare, endothelial dysfunction and structural anomalies (such as high levels of cell adhesion molecules or increased intima-media thickness in the carotid artery) are present in these patients before the clinical manifestations of vascular disease appear [10-12].
The aim of this study was to investigate whether a prothrombotic state exists in children with T1DM by assessing their Fg, PAI-1, and vWF:Ag levels and standard coagulation tests, such as platelet count, prothrombin time (PT), and activated partial thromboplastin time (aPTT). This investigation also attempted to determine if the studied molecules vary with time since T1DM was diagnosed and degree of glycemic control and to analyze the relationships between PAI-1 and the tested parameters.
Materials and methods
1. Study design/patient selection
This observational, analytic, and cross-sectional design included 35 patients with T1DM (20 males and 15 females) who visited the Department of Endocrinology of a pediatric hospital in TucumûÀn (Argentina) from March 2015 to December 2017. The mean age of diabetic patients was 11.0ôÝ2.5 years, and the time since diagnosis was 3.7ôÝ2.0 years, with no clinically demonstrable vascular complications; these patients were compared with 20 controls with similar age, sex, and body mass index (BMI). None of the T1DM patients or the controls had personal or first-degree family history of bleeding, thrombophilia, or thrombosis. All patients underwent a full clinical evaluation, including weight, height, BMI, duration of the disease, and any family history of diabetes and/or cardiovascular disease. Weight was measured using a mechanical platform scale (p-1003-k, Cam, Buenos Aires, Argentina) while the participants wore light clothing and no shoes. Height was determined by stadiometer (Seca 213, Seca, Hamburgo, Germany) while the participants stood with their ankles together, relaxed shoulders, and both arms at their sides. BMI was estimated using Quetelet's Index (weight/size2). Children with T1DM were being treated with long-acting insulin glargine (Lantus, Sanofi, Bs As, Argentina) at a dosage of 0.7ôÝ0.3 units/kg/day, and hyperglycemia was corrected with short-acting insulin (Apidra, Sanofi).
Absence of retinopathy was confirmed by ophthalmological evaluation using fundus examination. Nephropathy was ruled out by measuring urine albumin via immunoturbidimetric assay (DCA 2000, Siemens, US).
All children included in this protocol had normal lipid profile and blood pressure levels for their age and sex, according to the American Diabetes Association (ADA) criteria. Patients with inflammatory or infectious diseases, renal and hepatic diseases, acute or chronic diseases, malabsorption disorder, hypothyroidism, or other endocrine diseases were excluded from this protocol.
2. Biochemical parameters
Blood samples were obtained between 8 and 10 AM by venipuncture without a tourniquet after overnight fasting. Platelet count was assessed using anticoagulated blood collected with a 10% ethylenediamine tetraacetic acid additive using a blood cell counter (Sysmex KX 21, Kobe, Japan). Platelet-poor plasma was collected with 3.2% (0.109 M) sodium citrate at a 1:9 ratio and centrifuged at 3,000 rpm for 15 minutes. PT, aPTT, and Fg tests were immediately carried out using an ACL 300 coagulation analyzer (Diamond Diagnostics, Holliston, MA, USA). The PAI-1 and vWF:Ag plasma levels were measured by enzyme-linked immunosorbent assay (Asserachrom, Diagnostica Stago, Asniû´res-sur-Seine, France). Glycemic control was evaluated using hemoglobin A1c (HbA1c; DCA 2000, Siemens, USA), fasting blood glucose (enzymatic method, Wiener Lab, Rosario, Argentina), and capillary blood glucose levels. According to the recommendation by the ADA, HbA1c < 8% value was considered to represent good glycemic control (GGC), while HbA1c ãË 8% indicated poor glycemic control (PGC) [13].
3. Statistical analysis
Statistical analysis was performed using the IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). A Kolmogorov-Smirnov test was used to determine quantitative variable distribution. All data were expressed as frequency and percentage for categorical data and as meanôÝstandard deviation or median with Q1 and Q3 for numeric data. Differences in participant characteristics were compared across subgroups using a chi-square test for categorical variables and a T-test or Mann-Whitney U-test for continuous variables as appropriate. To compare the 2 groups, statistical hypothesis testing was applied for independent samples. The Pearson correlation coefficient was used to investigate correlations between parameters. A P-value <0.05 was considered statistically significant.
Results
The clinical and biochemical characteristics of the studied groups are shown in Table 1. Diabetic patients presented with significantly higher values of HbA1c, Fg, PAI-1, and vWF:Ag; however, standard coagulation tests did not show significant differences between the groups.
According to HbA1c value, 73% (n=26) of children with T1DM had PGC, and 27% (n=9) demonstrated GGC. Capillary blood glucose values were used to monitor the patients, who had average readings of 174 mg/dL before breakfast, 190 mg/dL before lunch, and 210 mg/dL before dinner. No significant differences were found in any hemostatic parameters studied between diabetic patients with GGC or PGC (Table 2).
Discussion
Vascular complications are the main causes of morbidity and mortality in diabetes. In patients with T1DM, different alterations of the coagulation system could be of interest, such as alteration in fibrin clot structure, changes in procoagulant molecules concentration, and reduction in fibrinolytic system activity. However, information on coagulation disorders and altered fibrinolysis in children with T1DM is limited [14,15].
The normal values for the global tests of PT and aPTT in our patients could be due to the sensitivity of the reagents and the coagulometer used. In children with T1DM, there were no differences in platelet count, PT, and aPTT in comparison with healthy controls; other authors have obtained similar results [16,17]. However, in diabetic adults, some authors have reported only shortening of aPTT, while others found shortening of PT; all agree that there is platelet dysfunction in diabetics in comparison to nondiabetic individuals [18-20].
The most interesting results of this study were the elevated levels of Fg, PAI-1, and vWF:Ag in diabetic children. Several investigations in adults and children with T1DM have suggested abnormalities in hemostasis. Carmassi et al. [16] found that patients with T1DM had elevated levels of Fg, Factor VII, thrombin and antithrombin complexes, and PAI-1, with a reduction in tissue plasminogen activator (tPA) activity in comparison to controls. Targher et al. [21] reported that, in comparison to healthy controls, the plasma levels of Fg, vWF:Ag, soluble intercellular adhesion molecule-1, and PAI-1 were remarkably higher in young people with T1DM, with no clinical evidence of macrovascular disease.
All these studies indicate hemostatic disorders in patients with T1DM. Several mechanisms contribute to the prothrombotic state in these patients, including endothelial dysfunction, hypercoagulability, and hypofibrinolysis. Further, chronic hyperglycemia promotes glycation of the proteins involved in fibrinolysis and affects clot structure, increasing its resistance to degradation by plasmin [22,23]. Moreover, hyperglycemia activates the metabolic pathways of polyol and protein kinase C, which increases oxidative stress. All these processes cause vascular damage that affects the hemostatic system [24,25].
Many researchers have emphasized the importance of GGC, particularly as diabetes duration increases, to reduce the risk of vascular complications [26]. Over time, the presence of PGC alters the levels of some metabolites, such as lipid profile (total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol), creatinine, uric acid, and some cytokines (interleukin [IL]-6, IL-17, interferon-ö°) [27-29]. However, changes in the hemostatic system have not been well studied in children. In this work, degree of glycemic control and duration of T1DM diagnosis did not significantly affect the hemostatic parameters evaluated. Similar findings were reported in a study of 84 Turkish T1DM children with a disease duration longer than 5 years, which showed that there was no correlation between serum PAI-1 level and disease duration or presence of microvascular complications [30]. In contrast, Zhao et al. [31] reported that PGC in adults with T1DM was correlated with increased Fg and shortening of PT and aPTT. Moreover, recent studies in young adults with T1DM found that chronic hyperglycemia and elevated HbA1c level were correlated with increased PAI-1, platelet aggregation, and protein C levels [32]. This divergence between glycemic control and hemostatic molecule levels suggests that more time is necessary to observe a change, or that there are other factors involved in adults (obesity, smoking, hypertension), which highlights the importance of GGC through the disease.
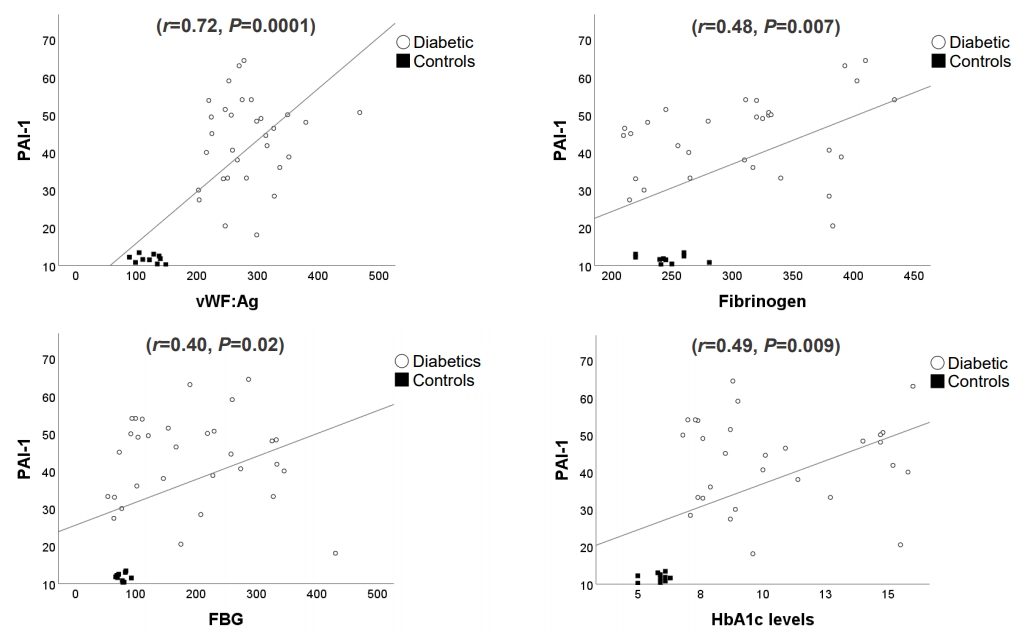
Fibrinolysis is a normal body process that remodels or degrades a blood clot. Fibrinolysis is activated by conversion of inactive plasminogen to plasmin (the enzyme responsible for cleaving fibrin) on the thrombus or cell surfaces by serine proteases such as tPA or urokinase plasminogen activator. Therefore, fibrinolysis is regulated highly [33]. This regulation is carried out primarily by PAI-1, which inhibits tPA. A systematic review of 52 epidemiological studies supported a relationship between PAI-1 and diabetes, which shows its potential as a biomarker of prothrombotic risk in this disease [34,35]. Our findings of elevated PAI-1 in children with T1DM and its positive correlation with levels of fasting blood glucose, HbA1c, Fg, and vWF:Ag suggest that elevated PAI-1 contributes to the hypercoagulability state seen in T1DM.
This work had some limitations. It was a cross-sectional design, which only allows for associations but no causality. The sample size was relatively small, and some results cannot be applied indiscriminately. Therefore, further studies are necessary to confirm our results and evaluate the clinical usefulness of these biomarkers to identify prothrombotic risk in diabetic children.
In brief, elevated levels of Fg, PAI-1, and vWF:Ag in pediatric patients with T1DM suggest a prothrombotic state. Children with T1DM face many years of hyperglycemia and the risk of early micro- and macrovascular complications. Therefore, an early detection of higher levels of these molecules could prevent or delay alterations beginning in childhood.